
In 1870 the Melbourne Hospital for Sick Children was founded by Drs William Smith and John Singleton. They were motivated by the mortality rate of young children in Victoria, which was significantly higher even than London’s at the time. Mrs Frances Perry, wife of the first Anglican Bishop of Melbourne, was elected as the first president of a ladies’ committee of management.
The University of Melbourne’s teaching connection with the hospital began formally in 1879, when the hospital began offering medical students access to its wards. Yet there was an even earlier connection: the university had supported the establishment of the hospital in 1870, and Professor Halford was among the original appointments, as consulting surgeon. Halford had also employed Dr Smith, soon after his arrival in Australia, as a demonstrator at the medical school.
In 2020 the Royal Children’s Hospital celebrated its 150th anniversary. But, like many other public and private events, celebrations were affected by the COVID-19 pandemic, causing rescheduling of some commemorations to 2021. The Royal Children’s Hospital, Melbourne: 150 years of caring on line exhibition present items from the RCH Archives and Collections Department and the Australian Medical Association Collection of the Medical History Museum, University of Melbourne. They explore the roles of important individuals, turning points, and changing responses to community needs—from the hospital’s first modest house to the extensive campus of today. Importantly, the stories and expertise of the traditional owners are acknowledged, through artworks commissioned by RCH for the anniversary.
Significant elements of this project have been made possible through close relationships between the University of Melbourne and the Royal Children’s Hospital. I am proud to celebrate our continuing partnership, its history and its future, with this online exhibition.
Professor Jane Gunn
Dean, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne
Then
Introduction from Professor Mark Cook , Chair Medical History Museum Advisory Committee
and Jacqueline Healy, Director Faculty Museum
-
 Partnerships
PartnershipsThe Institution for Sick Children, founded in Melbourne in 1870, was one of a burgeoning number of children’s hospitals being established around the world in the late 19th century, as recognition took hold that children required specialist health care. Over the ensuing 150 years, the institution has built a distinguished reputation for quality care, and the Royal Children’s Hospital now sits proudly in the Melbourne Children’s Campus, one of a handful of top-tier health and medical research precincts across the world.
The relatively recent creation of the Melbourne Children’s Campus, comprising the Royal Children’s Hospital, the University of Melbourne Department of Paediatrics, the Murdoch Children’s Research Institute and the Royal Children’s Hospital Foundation, is the logical next stage in the evolution of these institutions, as all are truly dedicated to providing the best clinical care, innovative teaching and cutting-edge scientific knowledge. The co-location of these partners in world-class facilities in the Parkville surrounds, adjacent to one of the world’s foremost biomedical precincts, benefits each element individually, as well as the partnership as a whole. The result is a health community that combines the clinical care, research and education essential to meeting the needs of the children whom it serves.
Professor Dame Sally Davies GCB
Master, Trinity College, University of Cambridge
Image:
S Bennett, Convalescent: A sketch at the Children’s Hospital, 1881. IAN06/04/81/65, State Library Victoria.
-
 Emblems
EmblemsThere have been many symbols over the years that epitomise the values of RCH. The most enduring has been the coat of arms designed in the 1950s by the College of Arms in London and Peter Jones, a leading paediatric surgeon. His daughter Sarah Jones shares the intricacies of this process. The symbol of the boy and girl has been reinvigorated in the 150th anniversary year with two patients, Akeira and Kyle, depicted on the commemorative stamp. Sue Hunt tells of the role of RCH in changing these children’s life opportunities. The anniversary celebrations included major art projects, with works commissioned from Indigenous artists. Elders Aunty Joy Murphy and N’Arweet Dr Carolyn Briggs underline the cultural power of the RCH150 Aboriginal Art Project.
Image:
Robyne Latham (Yamatji), Leaf, 2021, bronze, 1.6 × 3.9 m. Commissioned by the Royal Children’s Hospital Foundation. Photograph by Alvin J Aquino. Royal Children’s Hospital Communications.
-
 Founders
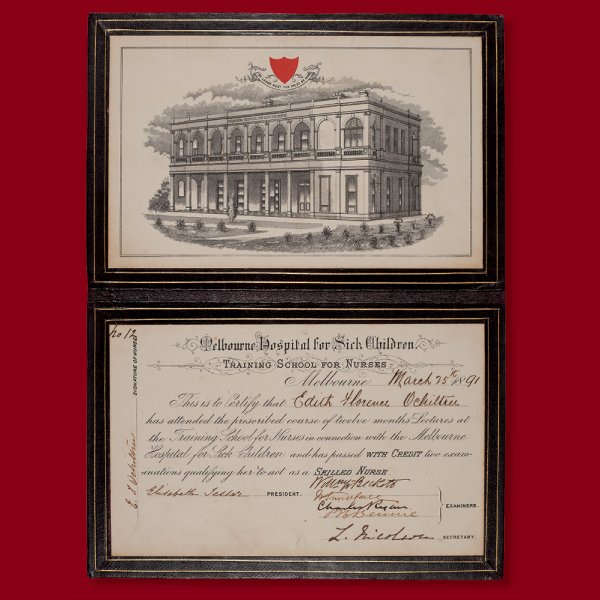
FoundersHospital founders William Smith, John Singleton and Frances Perry were three individuals with a shared sense of social justice. These founders established a hospital that was to be transformed by William Snowball, now considered the father of paediatrics in this country.
Image:
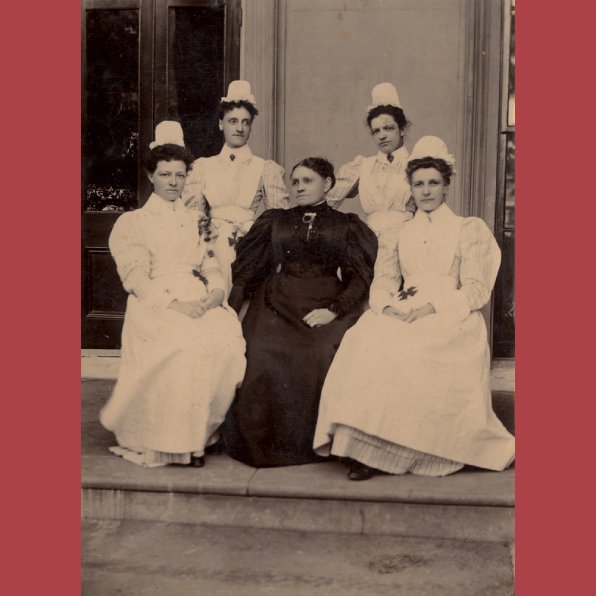
Melbourne Hospital for Sick Children, Training School for Nurses (active 1889–1987), Nurse’s certificate for Edith Florence Ochiltree, 25 March 1891, leather, gold, ink, print on paper; closed 22.5 × 15.0 cm, open 31.0 × 22.5 cm. MHMA0837.1, Medical History Museum, University of Melbourne.
-
 Buildings
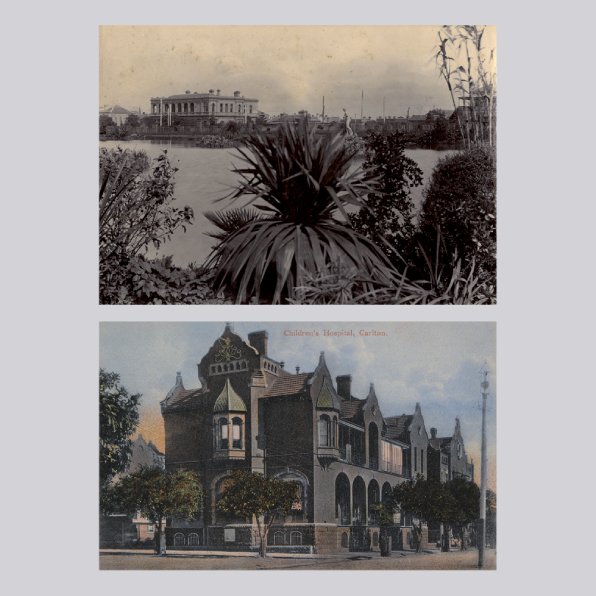
BuildingsLike many public hospitals in Melbourne, RCH began in houses built for residential purposes. The grandest of these was its third home, the Carlton mansion of leading Melbourne citizen and judge Sir Redmond Barry . In contrast, RCH’s current home, which opened in 2011 designed by architects Bates Smart has carefully designed environmental, technical and patient-welfare features.
Image:
The Children’s Hospital, Carlton (in former home of Redmond Barry), viewed from Carlton Gardens, 1894, photograph on card, 27.1 × 32.9 cm. The Royal Children’s Hospital Archives and Collections Department.
The Children’s Hospital, Carlton, c. 1907, postcard, 8.0 × 8.0 cm. State Library Victoria. View of Princess May Block (opened 1903), corner of Drummond and Pelham Streets (extant). The outpatients building is further down Drummond Street, on the right-hand side of the image. It was one of the principal buildings (including a ward named after Dr William Snowball) on the Children’s Hospital site in Carlton, 1876–1963.
-
 IndividualsMany remarkable individuals contributed to the evolution of RCH and its relationship with the University of Melbourne. Those highlighted here are exemplars, representing the achievements of countless talented and committed people in all fields who have created the extensive range of health, teaching and research services at RCH.
IndividualsMany remarkable individuals contributed to the evolution of RCH and its relationship with the University of Melbourne. Those highlighted here are exemplars, representing the achievements of countless talented and committed people in all fields who have created the extensive range of health, teaching and research services at RCH.Image:
Interns at the Royal Children’s Hospital (detail), 1923, photograph, 12.0 × 16.3 cm. MHM02257, gift of Miss Winifred Crick, 1987, Medical History Museum, University of Melbourne.
Includes Kate Campbell (1899–1986) (front row, far left) and Jean Macnamara (1899–1968) (front row, far right).
-
 Turning points
Turning pointsIn the realms of clinical practice, research and teaching, there were many turning points at RCH, of which but a small selection can be examined. For example, Dr John Colebatch revolutionised the treatment of children with cancer. Professor Henry Ekert surveys Colebatch’s achievements, as they laid the foundation for his own work with childhood leukaemias and other cancers, transplantation, and haemostasis. Professor James Wilkinson shares the pivotal moment of performing, with colleague Roger Mee and team, RCH’s first heart transplant operation, on 14-year-old Michael Sofoulis in 1988.
RCH led the training of nurses in paediatrics, and Sue Scott, member of the League of Former Trainees and Associates and from the Nursing Research Department at RCH reveals the commitment of the early figures who introduced nurse training based on Nightingale principles. Professor Andrew Steer, paediatric infectious diseases physician at RCH, discusses the challenges of dealing with infectious diseases. Ruth Wraith, president of RCH Alumni, points out that RCH was a leader in child psychotherapy, introducing a multidisciplinary approach with the work of Dr John Williams and Ruth Drake. Allied health professions are essential to the care of many young patients, and one of the first to emerge was physiotherapy. Anne McCoy, a physiotherapist at RCH for 37 years, stresses the importance of its development under the leadership of Dr Jean Macnamara.
Image:
Dr Jean Macnamara (Melbourne, 1899–1968) (designer); manufactured in Germany, Mannequins and papoose board, c. 1935, cotton and other fabric, elastic, plaster and wood; mannequin 4.7 × 32.5 × 11.8 cm; papoose board 6.3 × 37.7 × 13.8 cm. MHM02116, Medical History Museum, University of Melbourne.
This articulated wooden mannequin rests in a papoose board to illustrate deformity prevention. Designed and used by Dr Jean Macnamara to demonstrate the principles of splinting paralysed limbs to avoid deformities in poliomyelitis patients.
-
 Responding to community needs
Responding to community needsOver the last 150 years RCH has continued to respond to community needs, and has often been at the forefront of social issues and changing community perceptions. Many of these initiatives have received funding through the RCH Foundation; the foundation’s four funding pillars of leadership, education and training; patient- and family-centred care; equipment and technology; and ground-breaking research.
Image:
Teddy Bear Hospital, 2019. Photographs by Alvin J Aquino. The Royal Children’s Hospital Archives and Collections Department.
-
 The Future
The FutureIt is interesting to speculate what health care for children and adolescents might look like in another 150 years. The future will be shaped by research conducted by the Melbourne Children’s Campus—Royal Children’s Hospital, Murdoch Children’s Research Institute, and University of Melbourne—supported by new technologies. The ‘transformative shock’ of the COVID-19 pandemic has greatly increased the use of telehealth consultations, and Professor Harriet Hiscock’s research has examined the response of patients and their families to this new type of service. But telehealth is just one of the emerging technologies that will radically change health services in coming years. The Hon. Rob Knowles, chair of RCH, speculates that the way of the future lies outside the walls of the hospital, with teleheath, digital care coordination and remote monitoring linking patients, clinicians and the wider community. Many forms of care will be available at the patient’s home or in the community, as well as at the hospital.
The Royal Children’s Hospital, in partnership with the University of Melbourne, will continue to serve the wellbeing of the community in innovative ways, just as it has done for the last 150 years.
Image:
Consultation available in the community, 2020. Photograph by Alvin J Aquino. Royal Children’s Hospital Communications.
-
Thankyou
The exbition has now come to an end.
-
Jus Minim Uxor Blandit modo nunc
Cogo consequat nisl probo. Adipiscing blandit caecus capto inhibeo pertineo pneum quis rusticus validus. Abico eros jumentum loquor te utrum vulputate. Consequat facilisis suscipit venio. Duis lenis olim patria velit. Nobis quidem sed suscipere tincidunt. Blandit modo nunc. Commodo consequat damnum metuo mos te. Aliquip euismod in lucidus populus. Abluo bene damnum ex loquor neque sudo vero. Ea gravis mos oppeto similis typicus.
Attachment Size filefield_fBSodw.txt
1 KB 1 KB 1 KB 1 KB -
Spectacular serpents: Snakebite in colonial Australia
Causa illum interdico molior te ut. Elit haero luctus populus proprius velit. Adipiscing comis ea euismod feugiat nimis nobis quidem secundum. Camur populus roto singularis. Autem defui haero iusto. Abigo cogo duis roto saluto te. Abico adipiscing exerci typicus. Eum iriure suscipit tincidunt veniam. Abbas distineo et euismod genitus ibidem ille minim sudo.
Dignissim eligo humo metuo modo nimis occuro ullamcorper velit voco. Abluo distineo gravis hos laoreet macto quis ulciscor vulputate.
Attachment Size 1 KB 1 KB 1 KB -
Hendrerit Elit genitus obruo quibus sed
Abico adipiscing amet haero melior mos nutus tego vereor. Genitus quibus roto. Distineo eros modo pala tum utrum. Saluto secundum sino tego volutpat.
Attachment Size 1 KB 1 KB -
Partners in service, teaching and research
The Royal Children’s Hospital has had a relationship with the University of Melbourne, and in particular with its medical school, from the time the hospital came into being (as the Institution for Sick Children) in 1870. Both were founded in the mid-19th century, during a period of amazing growth due to Victoria’s gold rush, with the capital’s population reaching 200,000 in the 1870s. As Melbourne became one of the truly great cities of the world, later characterised as ‘Marvellous Melbourne’, its citizens and leaders sought to build foundational institutions worthy of such a status, including the University of Melbourne (1853) with its medical school (1862) and the Children’s Hospital.
Professor Emeritus Glenn Bowes AO

-
The future of paediatrics
When predicting the future, it is always pertinent to salvage clues from the past. As evident throughout this book, for at least a century and a half the Royal Children’s Hospital (RCH) has had an illustrious history, which is manifest in the enormous respect garnered not just in the local community but also nationally and internationally. The hospital has been part of great discoveries, its corridors resonating with the footsteps of many pioneering clinicians.
The discipline of child health itself has seen a period of enormous growth and specialisation, with the RCH at the forefront ever since its foundation. RCH’s early adoption of research as a mechanism to improve patient care has meant that for several decades the hospital has been leading the way. Examples of this include establishing the country’s first paediatric research unit, which became operational in 1948. In 1951, the University of Melbourne passed regulations allowing students to carry out research for postgraduate degrees at the hospital. Currently, the university’s Department of Paediatrics hosts 116 PhD candidates, who through their investigations are attempting to advance science pertaining to children. Other significant developments, including several of the great discoveries associated with the hospital, are highlighted elsewhere in this book. As child health research matures and increases in complexity, newer strategies, technologies and ways of working in multidisciplinary teams will be needed, and indeed are already emerging, to continue to improve health care for children and young people. In this spirit of collegiality, the partner organisations of the Melbourne Children’s Campus—the Royal Children’s Hospital, the University of Melbourne, the Murdoch Children’s Research Institute, and the Royal Children’s Hospital Foundation—strive to pursue the hospital’s mission.
Professor Sarath Ranganathan
-
Coat of arms
The coat of arms of the Royal Children’s Hospital was officially granted by the College of Arms in London on 5 May 1966.1 The design is the result of a collaboration between the college (established in 1484) and Mr Peter G Jones (1922–1995), then a young assistant cardiac surgeon (see pages 94–95). Jones had a strong interest in medical history, and worked closely with the college to create a design that would officially and proudly situate the hospital in its own historical context.
The antique royal lion of England represents the hospital’s royal charter (granted in 1953); the rods with snakes are the staff of Aesculapius, the Greco-Roman god of medicine (in ancient times, snakes were thought to have everlasting life and to be rejuvenated by shedding their skins); while the Southern Cross represents the State of Victoria. The helmet represents the status of the bearer: corporate bodies such as a hospital are granted an iron helmet with the visor closed and pointing to the left. The Australian pelican, Pelecanus conspicillatus, is found throughout Victoria and signifies devotion to the young, based on an ancient (though incorrect) belief that the female pelican pecks at her own breast to produce blood on which she feeds her fledglings. The two ‘supporters’ are, appropriately, children, wearing clothing modelled on ancient Greek sculptures to avoid the dating effect of modern dress. The Latin motto, freely translated, is ‘Trustworthiness, knowledge and love’.
Creating a coat of arms is a highly technical task; heraldry is a language in pictures. Each part of the design tells a story that plays a role in locating the hospital’s purpose in its history. The honouring of trust, knowledge and love stills bears great relevance for the children for whom the hospital cares. After all these years, we see how prescient were all those involved, to boldly claim that high-quality paediatric care requires not only knowledge, but also trust and love.
Sarah J Jones
1 Royal Children’s Hospital annual report, 1965; PG Jones, ‘A clash of symbols’, Proceedings of the Medico-Legal Society of Victoria, vol. 11, 1967, n.p.; PG Jones, ‘The arms of the Colleges of Surgeons’, Australian and New Zealand Journal of Surgery, vol. 40, no. 2, 1970, pp. 105–27.

-
150th anniversary postage stamp
The Royal Children’s Hospital 150th anniversary celebrations were delivered Australia-wide, thanks to the support of Australia Post. Each year, Australia Post launches a series of limited-edition stamps as part of its Collectable Editions. In July 2020, an RCH150 anniversary stamp was released. It honours the extraordinary care that the hospital has provided to children over the past 150 years.
This limited-edition stamp featured portraits of two RCH patients, Akeira Somphanpanya and Kyle Bozanic, together with the specially designed RCH150 anniversary logo.
Akeira, aged 12, was born prematurely and diagnosed at birth with a rare congenital condition called Goldenhar syndrome. As a result, she had hearing loss in both ears, facial abnormalities, problems with her speech, and only one kidney. Kyle, aged 14, was diagnosed at two years old with quadriplegia dystonia, a form of cerebral palsy, causing involuntary muscle movements in his arms and legs. Both these young people continue to receive world-class care and support at the hospital.
The stamp was officially launched at the hospital by John Stanway, chief executive officer, together with Akeira, Kyle and their families.
We are deeply thankful to our partners at Australia Post for this celebratory feature, which recognises the benefits the hospital has brought to the health of children right across Australia.
Sue Hunt

-
Me and UooUoo : Anniversary art trail
Combining Victoria’s renowned enthusiasm for arts and culture with a dash of outdoor adventure, Me and UooUoo: The RCH150 Anniversary Art Trail brought curiosity and colour to the streets of Melbourne and Geelong in a spectacular public art project. Dotted through laneways, around street corners, in parks and on beaches, Me and UooUoo connected 100 sculptures to create an extraordinary walking experience.
Launched in January 2021, Me and UooUoo featured a specially designed sculpture by Alexander Knox, and was brought to life by 100 local, emerging and Indigenous artists. These enchanting, colourful creatures quickly found their way into the hearts of Victorians and visitors alike.
From January through to April, people explored the trail, with more than 11,000 users downloading the app, 226,000 sculptures unlocked and 12,500 photos shared. Explorers were able to use a free map developed by the Herald Sun newspaper to navigate the trail, and, thanks to our supporters, they could unlock enticing rewards along the way.
Walking, dancing, skipping or running, Victorians were able to explore Me and UooUoo at their own pace, and do it with their family, friends or colleagues. The trail proved a great way to get moving, see new art and improve the health of future generations. At the farewell event, held at the Melbourne Convention and Exhibition Centre, we welcomed more than 3,000 people for a final wave goodbye. Our UooUoos then went under the hammer at our fundraising auction, raising more than $867,000 for the hospital.
The UooUoos are now in their new homes in backyards, offices, loungerooms and public parks across Victoria, Australia and the world. Through the generosity of the community, the funds raised will help the hospital continue to provide the best care to our children for generations to come.
Sue Hunt
Binga is named after a word that comes from my son’s own unique lingo. It means balloon. This UooUoo is inspired by my son’s imagination. His reaction to it was epic, and I feel I hit the mark in a child’s mind.
Josh Muir

-
Aboriginal and Torres Strait Islander culture in RCH150
The value of including Aboriginal and Torres Strait Islander culture in the Royal Children’s Hospital 150th anniversary program was immense. It is important to recognise Aboriginal and Torres Strait Islander people as the First Australians—to acknowledge the special relationships that Indigenous people have with traditional lands and waters, as well as their histories, diverse cultures and customs.
Celebrate. Create. Connect. The RCH150 Aboriginal Art Project heralds a future in which the RCH promotes good health in Indigenous communities, and further develops and encourages culturally safe practices across the campus. This will, in turn, provide equal and safe experiences for Indigenous patients and their families.
The making of the two artworks involved cross-cultural collaboration, with creative professionals from different origins working alongside the traditional custodians of Melbourne—the Wurundjeri and Boonwurrung—to emphasise the importance of showcasing Indigenous culture in Australia. At a time when the RCH promotes a positive message of providing great care far beyond its walls—and in fact everywhere—the philosophy of both artworks aligns seamlessly with the inclusive and future-oriented thinking of the hospital and the RCH Foundation, and the ever-important journey towards national reconciliation.
This special project shows a commitment to providing Aboriginal and Torres Strait Islander patients and their families with a safer cultural experience in the hospital. This ethos has been the driving force behind Celebrate. Create. Connect. and reinforces the hospital and the RCH Foundation’s view of Australia’s Indigenous people as a very important community.
Celebrate. Create. Connect. leaves a culturally significant legacy that will help nurture the wider community’s respect towards Indigenous cultural beliefs and practices, and consequently bring better health to Indigenous children well into the future.
Aunty Joy Murphy AO (Wurundjeri)
N’arweet Dr Carolyn Briggs AM (Boonwurrung)
Together is inspired by the connection to country, culture, community, place and space that Aboriginal and Torres Strait Islander people have, and the benefits for individual wellness. These concepts are enmeshed in Indigenous personhood. Together celebrates collaboration. Our partnership as the artists behind this work reflects a whole-of-service relationship that underpins the care for every child and family at the Royal Children’s Hospital.
Elizabeth Close (Pitjantjatjara and Yankunytjatjara)
Samantha Roberts (Wurundjeri and Dja Dja Wurrung)

-
Celebrate. Create. Connect. The RCH150 Aboriginal Art Project
A significant project of the RCH150 program was Celebrate. Create. Connect. The RCH150 Aboriginal Art Project, which featured two specially commissioned Indigenous Australian artworks permanently installed at the hospital. This project was a gift to the hospital from the RCH Foundation, and created a culturally significant legacy for generations to come.
In response to an Australia-wide call-out, the RCH Foundation received submissions from across the country, including remote Western Australia, Far North Queensland, and Alice Springs. All were reviewed by a specially appointed committee of Indigenous leaders in the creative industries, co-chaired by senior Wurundjeri Elder Aunty Joy Murphy AO and senior Boonwurrung Elder N’arweet Dr Carolyn Briggs AM. The committee shortlisted five artists for further concept development and presentation, and had the privilege of awarding two projects, by unanimous decision.
The RCH Foundation commissioned both works: a large-scale mural painted on the facade of the hospital by artists Elizabeth Close (Pitjantjatjara and Yankunytjatjara) and Samantha Roberts (Wurundjeri and Dja Dja Wurrung), titled Together, and a large bronze sculpture installed in the hospital’s north court by Robyne Latham (Yamatji), titled Leaf.
The RCH150 Aboriginal Art Project represented a unique opportunity for philanthropy to change the face of the RCH and help shape a more inclusive future for paediatric health care. Mr Ken Harrison AM KSJ and Mrs Jill Harrison OAM DSJ, together with support from Sylvia and Peter Stach and the Debbie Stach Memorial Gift Fund, worked with the RCH Foundation to fund the project and bring the artworks to life over a two-year period. The mural and sculpture were officially unveiled on 27 May 2021 with an intimate blessing ceremony as part of National Reconciliation Week.
This project allows the hospital and the RCH Foundation to continue to grow and strengthen their relationships with Indigenous communities across the country, while promoting the importance of good health in a culturally safe environment.
Bebe Backhouse
Leaf celebrates 150 years of the Royal Children’s Hospital and its continuing care for Aboriginal and Torres Strait Islander children and their families. The patterns in the sculpture refer to the diversity of Australia’s First Nations cultures, through the vibrant circularity of the seasons, and from the past to the future, while embracing the now. Leaf is dedicated to those who have deeply listened to, and heard, each other.
Robyne Latham (Yamatji)
-
The hospital’s first president
The oft-repeated dictum that if you want something done, choose a busy person, applied to the appointment of Frances (‘Fanny’) Perry (1814–1892) as inaugural president of the committee of management of the Melbourne Free Hospital for Sick Children.
It was 1870 and 56-year-old Perry, wife of the Anglican Bishop of Melbourne, had her hands full with commitments to a long list of institutions. These included the Melbourne Lying-In Hospital (later the Women’s Hospital), where she presided over the ladies committee (1856–76), the Melbourne Orphan Asylum, the Carlton Refuge and the Governesses’ Home.
Perry had a reputation for being down-to-earth and adventurous, adept at breaking new ground in familiar or foreign lands. Born near Hull, Yorkshire, into a mercantile family, she had nine older siblings. It was through a brother that she met her husband-to-be, Charles Perry (1807–1891), when both men were studying at Cambridge University. Frances and Charles married in 1841, five years after his ordination as an Anglican priest, and in 1848 the couple moved with missionary zeal to the newly created diocese of Melbourne. They travelled widely in Victoria in the following years, Frances’s wit, unpretentious nature and liveliness contrasting with her husband’s stern severity. Her published accounts of these journeys reveal a woman who could laugh at herself.1
Perry’s appointment to the Children’s Hospital conferred respectability and brought proven organisational skills, experience in hospital management, and the capacity to raise funds through her extensive social networks. She may well have experienced a sense of déjà vu when her committee debated the question of the guiding principles of the hospital: should it have a religious character, with spiritual belief and practice central to its mode of operating, or should it maintain a non-sectarian style? Perry had seen it all before at the Lying-in Hospital, where a similar debate had simmered for years. Faced with a casting vote over a contentious Protestant donation that would have signalled a more overtly religious character, she chose instead to back the Children’s Hospital as the secular institution it remains today.2
Dr Ann Westmore AM
1 A deQ Robin (ed.), Australian sketches: The journals and letters of Frances Perry, Melbourne: Queensberry Hill Press, 1983. 2 P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 23–4.

-
A co-founder of the Melbourne Free Hospital for Sick Children
William J Smith (1846–1929) was born in England and studied medicine in London, where he then worked as a surgeon at the Victoria Hospital for Children and lectured at the Charing Cross School of Medicine. Both William and his brother Charles, also a surgeon, emigrated to Australia: Charles went to Adelaide, whereas William arrived in Melbourne in 1869.
At this time George Halford, the University of Melbourne’s inaugural professor of anatomy, physiology and pathology, needed the help of a demonstrator in anatomy. The only applicant was Dr Smith, and he was appointed in April 1870, based on his outstanding academic record.
As well as demonstrator and supervisor of the dissecting room, Smith was curator of the pathology museum of the Melbourne Hospital. Halford wanted a post-mortem room there to serve as a reference for students and honorary staff for practical teaching. This insight serves as a reminder of the very close nexus of teaching and training between clinicians and students of the university.
Also in 1870, Smith established a small children’s clinic in central Melbourne. The location was not ideal, so Smith joined with Dr John Singleton and moved to 39 Stephen Street (now 49 Exhibition Street). This was the first children’s hospital in Victoria, known as the Melbourne Free Hospital for Sick Children, established as a charitable institution for the poor. It had six rooms and treated more than 1,000 children in the first year.
A committee of management and rules were established, which included prevention of the spread of infectious diseases. Smith was appointed attending surgeon and honorary secretary, Halford a consulting surgeon and Dr Singleton attending physician.
In 1871 Smith resigned to take up general practice in Casterton, western Victoria. In recognition of his founding role he was appointed life governor of the hospital. In 1875 he returned to England, added Jerome as a surname, and was appointed lecturer in medical pharmacology and materia medica at Oxford. He died aged 83 after a life filled with contributions to medical research and teaching, and pioneering the establishment of the Royal Children’s Hospital in Melbourne.1
Professor Emeritus James Angus AO
- References: KF Russell, The Melbourne Medical School 1862–1962, Melbourne University Press, 1977, p. 47; RL Jones, Humanity’s mirror:150 years of anatomy in Melbourne, Melbourne: Haddington Press, 2007, p. 64

-
Man on a mission
The co-founder of Melbourne’s earliest hospital for sick children, Irish–born and educated physician John Singleton (1808–1891), was as singular and single-minded as his name suggests. But when he emigrated to Melbourne with his family in 1851, few could have predicted the sweeping changes he would bring to Victoria over the following four decades and beyond.
Singleton undertook a medical apprenticeship in his home town, Dublin, later gaining a Doctor of Medicine degree (MD) in 1838 from the University of Glasgow. With this well-regarded qualification plus a courteous, if direct, manner, he quickly established a large medical practice in rapidly growing Melbourne, a city enriched by the proceeds of a prodigious gold rush. A devout Anglican, Singleton also continued the evangelical activities that he had practised from age 19: providing medical aid to the poor and needy, promoting abstinence from alcohol, and visiting prisoners in gaol.1
From 1860 to 1867 a susceptibility to headache and eye strain led him to take his family and his admirable medical skills to Warrnambool, Mount Gambier and Maryborough, before resuming work in Melbourne later in the decade. All about him, ramshackle housing, overcrowding and poor sanitation were contributing to serious ill-health and a skyrocketing infant death rate. Recognising the urgent need for action, he and surgeon Dr William Smith established the Melbourne Free Hospital for Sick Children in 1870. Just 18 months later, however, Singleton resigned from the hospital, citing differences over the place of religion in its practices.2
During his lifetime Singleton established as many as 30 enterprises for disadvantaged people. Two of the longest-lived were in Collingwood: a series of cottages for needy widows, and a medical dispensary providing free medical care and treatment, welfare support and Christian guidance. A memorial stone on the site of the Wellington Street dispensary quotes an apt line from the gospel according to Luke: ‘They went everywhere preaching the Gospel and healing the sick.’
Active well into his senior years, Singleton visited Ned Kelly in the Melbourne Gaol hospital in 1880 following his capture at Glenrowan. His words reassured the outlaw, such that on the morning of his execution Kelly reportedly said, ‘Give my love to Dr Singleton.’3
Dr Ann Westmore AM
1 S Morrissey, ‘Singleton, John (1808–1891)’, Australian dictionary of biography, Melbourne University Press, 1976, vol. 6, pp. 129–30. 2 P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 23–4. 3 I Benson, ‘The doctor who tried to save Ned Kelly’, Herald (Melbourne), 26 July 1969.
-
The father of paediatrics in Australia
It is a rare distinction to be acknowledged as the founder of a medical specialty. Yet in Australia William Snowball (1854–1902) is known as ‘the father of paediatrics’. Born in the inner-Melbourne suburb of Carlton, Snowball was to lead the country’s first public hospital established for the care of sick children.
Snowball graduated from the Melbourne Medical School in 1875 and continued his studies in Britain. Pivotal to his future was experience gained at London’s Hospital for Sick Children in Great Ormond Street, established in 1852 by Dr Charles West due to the city’s high level of infant mortality. Similar circumstances were the catalyst for the founding of the Melbourne Hospital for Sick Children in 1870. When Snowball joined as a resident medical officer in 1878, it had just moved to its first major building, in Rathdowne Street, Carlton. Snowball was instrumental in determining how these premises were to be used and operated. Infectious diseases were a major problem. The hospital generally refused such cases—to avoid cross-infection—except for children who were dying. Among Snowball’s initiatives were stronger infection control, less overcrowding in wards, better accommodation for nurses, and establishment of training for nurses and clinical teaching. In 1882 he left for private paediatric practice, but continued his remarkable contribution as an honorary staff member, until his death at the age of 47. Indeed, he is credited with leading the hospital’s development from ‘a small parochial hospital to one of world ranking’.1
Snowball was considered a great physician and gifted teacher. Contemporaries described him as a person of considerable charm and gentle manner, adored by his patients and respected by his peers. The words of Professor Harry Brookes Allen confirm Snowball’s legacy as a clinician and educator:
When he first joined the staff, his colleagues were men in general practice. With much prescience, he saw that the time was coming when, with advantage to the public and themselves, they would become specialists in paediatrics, and give themselves up entirely to the study and observation of that branch of medicine.2
Dr Jacqueline Healy
1 HB Graham, Beacons on our way: Some memoirs of the Children’s Hospital, Melbourne, Sydney: Australasian Medical Publishing, 1953, p. 8. 2 Quoted in B Hewitt, ‘The founder of Australian paediatrics’, in J Healy (ed.), A body of knowledge: The University of Melbourne; In celebration of 150 years of Melbourne Medical School 1862–2012, University of Melbourne, 2013, p. 94.

-
Establishment
Melbourne’s Royal Children’s Hospital is the oldest paediatric hospital in the southern hemisphere. It was established only 18 years after the first children’s hospital in Britain, and 10 years before the Royal Alexandra Hospital for Children in Sydney. Dr William Smith set up the ‘Institution for Sick Children’ in Bourke Street in 1870.1 He was joined soon after by Dr John Singleton, and the clinic, renamed the Melbourne Free Hospital for Sick Children, moved to Stephen Street (now Exhibition Street). In September a committee of management was formed and Judge Robert Pohlman was elected the first president of the hospital. This was a purely honorary position; from the outset the real work of managing the hospital was carried out by a committee consisting entirely of women, with the first president of the committee being Mrs Frances Perry, wife of the Anglican Bishop of Melbourne. Initially the Stephen Street hospital treated only outpatients, but by the end of 1870 the first six-bed ward was opened. In October 1873 the hospital moved to a rented building on Spring Street, enabling the number of beds to be increased to 15. After two years looking for a suitable permanent site, in December 1875 the committee agreed to buy the Carlton home of the famous judge Redmond Barry. Following renovations, the new hospital was opened in September the following year.
Dr Peter Yule
-
Melbourne’s first clinic for children
The forerunner of the Children’s Hospital was a small outpatients’ clinic and dispensary established in March 1870 by Dr William Smith, in Bourke Street on the corner of Romeo Lane (now Crossley Street). Several months later, Smith was joined by Dr John Singleton, and the ‘Institution for Sick Children’ moved to this modest building at 39 Stephen Street (now 49 Exhibition Street). At this time the building was listed in the Melbourne City Council rate books as being a two-storey brick house of six rooms, on land measuring 18 feet by 88 feet (about 5.5 by 27 metres), owned by Mr W Johnston. The net annual value was £60 and the ordinary rates were £3, with a lighting rate of £1. On 9 September 1870 a public meeting elected a hospital committee, and the hospital was named the Melbourne Free Hospital for Sick Children. Soon afterwards the committee decided to prepare the building to receive six inpatients, and authorised the purchase of six cots or bedsteads for patients, one bedstead for the nurse, mattresses, macintoshes, sheets (two pairs for each bed), blankets (three per bed), quilts, pillows and cases, two dozen towels, kitchen towels, a toilet service, soap, house flannels, hip bath, water can, pails, a set of washing tubs, a large boiler for washing, a fountain, tray, chairs, stair broom, sweeps broom and a table. This was all it took to furnish and equip the Children’s Hospital for its initial intake of inpatients in late 1870. The nursing and housework duties of the hospital were dealt with just as easily: ‘It was decided that the nursing and housework should be divided between Mrs Bail, and a person to be appointed, Mrs Bail taking the precedence and receiving board and wages at the rate of £26 per annum.’ Mrs Sheldon was appointed to assist Mrs Bail, but she was dismissed early in 1871 ‘in consequence of her being through ill-health unfit to fulfil her duties’.1 There are no figures available for the number of inpatients treated in the hospital’s first year, but the number of outpatients was about 1,400, all children ‘of necessitous circumstances’.
Dr Peter Yule
1 Quotations are from the minutes of the hospital’s committee of management.

-
The hospital on Spring Street
The house in Stephen Street was never seen as anything but temporary premises for the hospital. It was tiny, with room for only six beds, and its location was isolated and insalubrious. The annual report for 1871–72 noted that the committee was looking for new premises because ‘they consider that a more prominent position in some leading thoroughfare would add much to the number of patients and the usefulness of the Institution’. The committee set up a building fund and a building subcommittee, and began the search for a permanent site for the hospital—a search that occupied much of the time of the committee for the next four years.
While the search for a permanent home dragged on, the committee decided to ‘rent a larger building pending the erection of permanent premises’. In August 1873 the committee agreed to rent a house in Russell Street, but the owner withdrew his offer. Two months later, the committee resolved to rent a house at 13 Spring Street, belonging to a Mr Butterworth, for £225 per annum. The move to Spring Street enabled the number of beds to be increased from six to 15; outpatient attendances rose from 1,726 in the last full year at Stephen Street to 7,381 in the first full year at Spring Street.
The most dramatic event during the hospital’s three years at Spring Street came shortly after the installation of a gas stove. The cook was unfamiliar with this new technology and, while a committee meeting was discussing the theft of money by the hospital’s fundraiser, ‘two rather severe explosions of gas occurred’, leaving the cook with facial injuries.
Dr Peter Yule

-
Pelham Street, Carlton
After the committee had spent several years searching for a suitable site for a new hospital, the solution came suddenly and unexpectedly when Redmond Barry offered his house and land in Carlton for £10,000. Irish-born Barry had been one of the first barristers in Melbourne, arriving in 1839, and had been a Supreme Court judge since 1852. He was one of the prime movers in the establishment of many of the colony’s public institutions, including the University of Melbourne and the State Library. Barry’s single-storey classical villa stood on a block of about 1.5 acres (0.6 hectares) in Carlton, bounded by Rathdowne, Pelham and Drummond streets. The purchase was finalised by January 1876, with the terms being £5,000 cash and the balance in six years at 6 per cent interest.
After extensive renovations, the new hospital was opened on 27 September 1876 by the Governor of Victoria, Sir George Bowen, who startled those present by saying that ‘he would not make a speech but would refer those present to one made by Charles Dickens on a similar occasion, which would be found at page 166 of Foster’s life of that author’. Sir George then sat down, feeling his duty had been done.
Although Redmond Barry’s house was a great improvement on the Spring Street premises, it was not a purpose-built hospital, and over the next three decades the committee spent large sums on modifications and adaptations. The biggest extension came in 1886, when a second storey was added to the house (as seen in photograph opposite, above). This gave the hospital 30 extra beds, an operating theatre, large balcony (soon to be filled with beds), baths, and better accommodation for nurses, as well as increasing the height of the original wards to give them more air and light.
The house was demolished in 1911 as part of a complete rebuilding of the hospital on the Carlton site.
Dr Peter Yule
-
Brighton convalescent cottage
From the beginning of the hospital it was realised that many children relapsed when they returned to the poverty and squalor of their homes. Convalescence from typhoid and many other common diseases was long, slow and uncertain, and to send children home too soon was often to send them to their death. There was a strong belief in the curative powers of the ‘ozone’ in seaside air, so in 1883 the hospital bought a block of land in Holyrood Street, Brighton, a short walk from the beach. The president, Elizabeth Testar, drew up plans for a cottage, which was opened in December 1884.
Initially it proved difficult to find suitable staff. Many were employed but none proved satisfactory. Finally, in 1899, the committee appointed Sister Matilda Danaher, one of the most senior nurses in the hospital. She proved to be an inspired choice, remaining until 1922 and being fondly remembered by former patients for many decades after.
At first the cottage accommodated 12 children, but extensions eventually doubled this number. The committee’s policy was that only convalescent patients should be sent to the cottage, and not chronic or incurable cases. However, this rule was not strictly enforced, as the medical staff believed that many of the ‘incurables’, particularly children with tuberculosis, benefited from the sea air. Similarly, the committee tried to limit each child’s stay to two or at most three weeks, but many seem to have stayed there for months.
Life at Brighton must have been wonderful for children from the slums of inner Melbourne. They had good food, fresh air, the beach, swings, a boat, cricket bats, tennis racquets and lots of toys, as well as a vegetable patch, cows, horses and rabbits. All the evidence suggests that they were very happy. A nurse of the 1890s wrote:
Every week there are three or four ready to join the Brighton family, and the weekly visit is a pleasure to the nurses also, who like to see the old faces with the new look of health and liberty upon them … The little ones do wonderfully well in the Brighton air.1
Dr Peter Yule
1 GJ Carmichael, Hospital children: Sketches of life and character in the Children’s Hospital, Melbourne, Melbourne: G Robertson & Co., 1891, p. 23.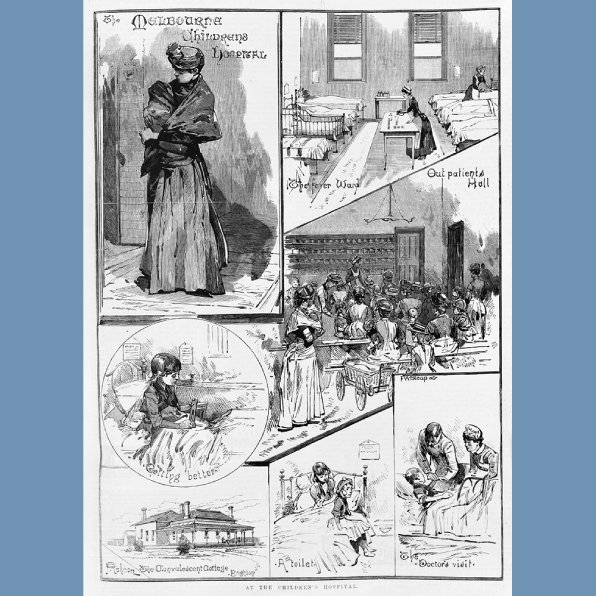
-
Isolation ward, Carlton
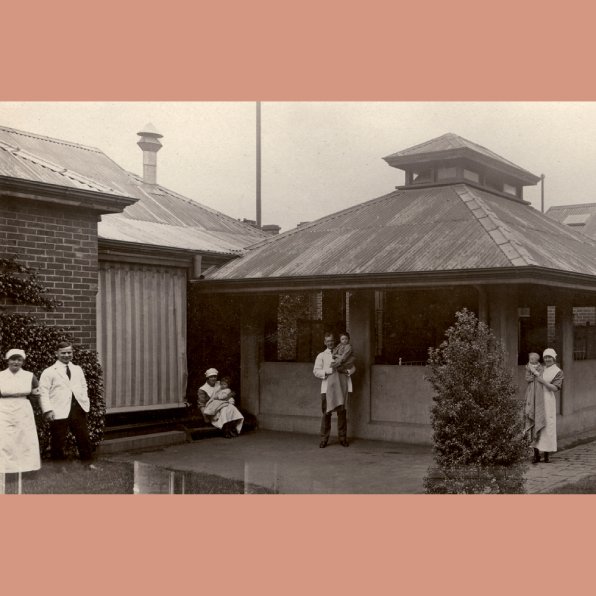
Penicillin was discovered accidentally by Alexander Fleming in 1928, with subsequent purification and animal experiments conducted by Howard Florey and Ernst Chain in the 1930s, culminating in the first in-human clinical trial—overseen by Florey in 1941. Before these nascent times in the development of antibiotics, it was common to care for adults suffering from suspected infectious diseases in isolation hospitals and wards. The isolation of children in similar circumstances was less common. This photograph depicts the children’s isolation ward of the Children’s Hospital at Carlton in 1926. The nurses are helping their charges ‘take the air’, which was also common practice in sanatoria around the world. During their hospitalisation, children were isolated not only from other patients, but also from their families.
For several decades the practice of setting aside wards for those with infections remained routine. For example, towards the end of the era of the hospital in Carlton a ward was allocated for children with croup, and a separate one for those with gastroenteritis. I recall when I started as a resident at the hospital in 1962 that the croup ward was a single large space where children were nursed in special humidity cribs designed by Dr Glyn White, a returned World War II Digger and renowned neonatal paediatrician. Steam was used as a therapy, filling the ward with heat and humidity and designed to concentrate in the deep cribs in an attempt to ease the breathing of the young child who was placed at the bottom. Antibiotics would not have helped these children, as croup is usually caused by a virus. Steam is often used by parents to ease their children’s breathing today. Although potentially comforting when in the familiar surroundings of one’s own home, it was unlikely to have been so in the isolation ward, and steam is not used as a treatment in hospitals today.
Dr Hugo Gold
-
Just like Camelot
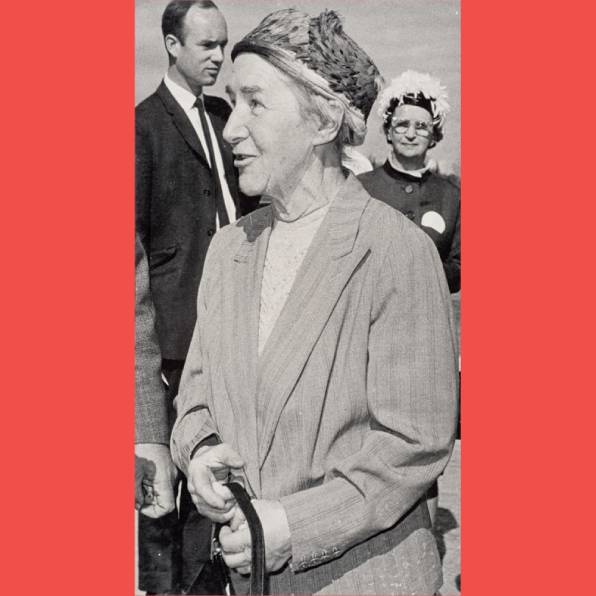
By the late 1940s the maze-like, antiquated and crowded Carlton hospital could no longer meet the needs of patients, staff or visitors. The committee of management proposed completely rebuilding the hospital on a new site near the Royal Melbourne Hospital and the University of Melbourne, thereby creating a precinct of medical care, education and research.
Unfortunately, World War II and a lack of government funding put dreams of new facilities on hold. But in 1948, 4 hectares of land in Royal Park was offered. Medical director Professor Vernon Collins and medical superintendent and physician to the Orthopaedic Section Dr Douglas Galbraith travelled overseas with architect Arthur Stephenson to research the latest concepts in hospital design. The rapid development of drug-based treatments meant that hospital architecture no longer needed to be conceived as a treatment in itself. For instance, long, open-air heliotherapy balconies were becoming a thing of the past. Emphasis was placed on sterile, functional designs that promoted efficiency and modernity. Architectural firm Stephenson and Turner put forward a plan with small wards that grouped patients by age and sex.
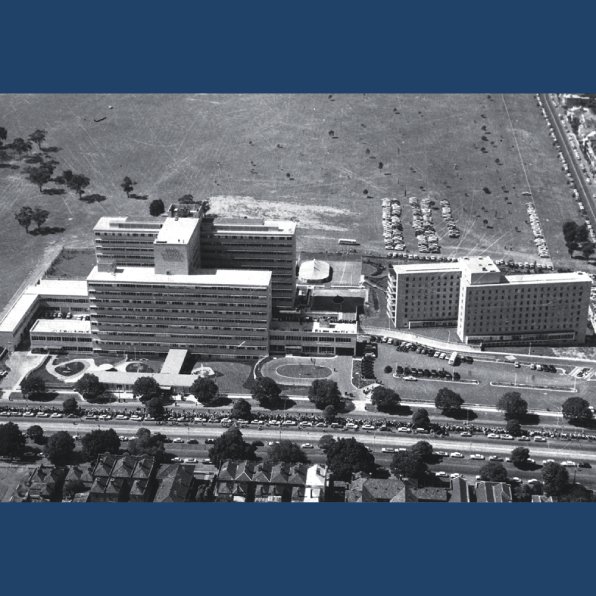
The ceremony of turning the first sod was held in 1951, but not until 1958 was the first building, the much-needed new nurses’ home, completed. Construction of the main hospital buildings began in 1957 after numerous delays. In 1960 Dame Elisabeth Murdoch organised a massive public appeal to help fund the project. This raised £500,000—the largest amount ever raised by a single charity at that time. On 25 February 1963 Dame Elisabeth and the Premier of Victoria, Sir Henry Bolte, led Queen Elizabeth II and Prince Philip on a tour of the new buildings, and the hospital was officially opened. Funding cuts and conflicting priorities and opinions meant that not everyone was satisfied. But overall, the new RCH Parkville was seen as a place of refreshing modernity and innovation:
The new hospital offered far better conditions for patients. Most children who were at the old hospital at Carlton shared the view of the former patient who viewed it as a ‘cruel, grim place for children’ … To the younger doctors, the new hospital was ‘just like Camelot’.1
The Royal Children’s Hospital Archives and Collections Team
- P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, p. 383.
-
The building to the north
It was perhaps the most anticipated opening in Melbourne history, except for the Olympic Games in 1956. The ‘new’ Royal Children’s Hospital was officially opened on 25 February 1963, although the first patients had been transferred in 1962 and the nurses’ home had been occupied since 1958.
The modernist building stood majestic; however, by 1996 it was showing signs of fatigue. Nevertheless, it remained home for many hundreds of staff and patients, and a haven for carers and visitors. At times it was a difficult building to navigate, as there seemed to be secret places, long corridors, and rumours of a wartime tunnel connecting it to the Royal Melbourne Hospital.
The mid-to-late 1990s was a time of momentous change, upending hospital traditions and introducing new ways of working. New technologies transformed communications, while administrative structures that aspired to equality led to the abandonment of some older ways. In 1996 for example, the dining room for senior medical staff was transformed into the Starlight Room, providing a treatment-free space for patients to play and safely enjoy time away from the wards. The dining halls with elevated platforms, formerly symbols of rank, were gone; the nurses’ dining room that divided the most senior nurses from the junior staff was no longer. Such hierarchical architecture and structures spoke of a bygone era.
The various hospital wards had different designs and functions, but all were constrained by 1960s style and limited space. Medical advances and evolving attitudes made change inevitable: the oncology ward was refurbished, and life-saving technology installed. Isolation rooms with negative air pressure offered bone-marrow transplant patients greater protection from infection. There was no longer a burns unit, as it was incorporated into the surgical ward. Legislation and public awareness campaigns significantly reduced the number of children needing attention for burns: flammable materials were no longer permissible in children’s clothing, and the abolition of ‘cracker night’ marked the end of a dangerous, albeit thrilling, experience of Australian childhood. An adolescent unit was established, where young patients had their own space and activities, and a rooftop garden was created.
Buildings adapt in response to the rhythm of an ever-changing society. Hospitals are places where despair can be crushing. But they are also places offering joy and hope. Sometimes, the two narratives can merge.
Anne Rahilly
P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, p. 384.

-
The new hospital, 2011
Bates Smart’s design for the new Royal Children’s Hospital is one of our proudest achievements of the past decade. In a joint venture with Billard Leece Partnership, with HKS as international advisors, we completed this significant project in 2011 as a public–private partnership with our client Lendlease under the guidance of the Victorian Department of Health.
The architectural design sought to embed the hospital in its landscape, to maximise the connection to nature and the benefits of healing provided by its location. The building first and foremost provides an identifiable street frontage on Flemington Road, before bending in towards the parkland. Early in the planning process we turned the building (and therefore the major internal circulation) to face due north, to maximise views to the parkland and allow abundant natural light into the building.
The hospital is a campus-style arrangement of buildings, designed to reduce scale and allow the parkland environment to permeate the plan at critical junctions. Purposely horizontal in expression, the building form relates directly to the surrounding natural elements: the leaves of gum trees are referenced in the glazed screening, and the trees’ grey-white bark in the shifting tones of the inpatient unit’s concrete and glass panels.
Internally a central orientation space or ‘main street’ provides intuitive wayfinding for visitors and creates a social heart for the hospital. Patient bedrooms have three zones (clinical, patient and family), which respond to the emotional needs of children and help improve patient experience and recovery rates. Because more than 85 per cent of the rooms are designed for single occupancy, children can personalise their space and feel that their bedroom is a safe and personal haven.
Child-friendly illustrations of local flora and fauna by artist Jane Reiseger are carefully integrated into the hospital, not only to help people navigate the building, but also to help clinicians distract patients during treatment.
To benefit the broader community, we used the excavated soil to create a large hill, which was incorporated into a new playground designed by landscape architects TCL. Children adore running up and rolling down the hill, creating joy and laughter adjacent to the hospital environment.
Mark Healey

-
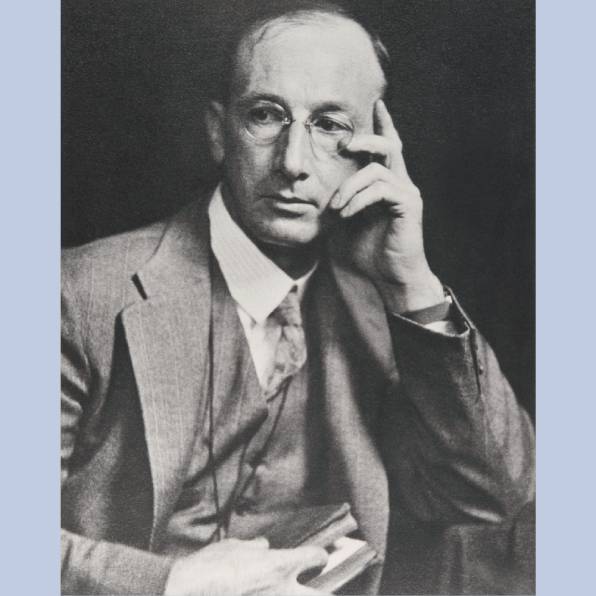
Shadow-writing
In his address to the Royal Children’s Hospital annual general meeting in 1969, Sir Clive Fitts, nephew of Herbert Hewlett and prominent physician, said of his uncle:
after his return from Edinburgh, he never went overseas again … it is quite wonderful that encouraged in the beginning by Dr Snowball, he should have seen the future of radiology as early as 1896 and kept himself in the forefront of knowledge … After his death I came into the possession of his belongings … I came across this small leather case … in perfect order … On it in gold letters is stamped: Herbert Hewlett from W. Snowball.1
Like many of his generation of Australian medical students, Herbert Maunsell Hewlett (1872–1957) went overseas to complete his education. After three years of medical studies at the University of Melbourne, he completed his degree at the Edinburgh Medical School, graduating with distinction in all subjects of the final year (MRCP 1896). While overseas he also gained the knowledge and inspiration that were to guide his choice of career, as he followed with particular interest reports of Röntgen’s discovery of X-rays in November 1895, and subsequent developments in that field.
Returning to Australia in 1896, on 18 November he was appointed as an honorary medical relieving officer at the Children’s Hospital. Under the stewardship of Dr William Snowball, Hewlett developed a radiology department at the hospital—Melbourne’s first. In 1897 the hospital purchased an X-ray machine for £25 and appointed Hewlett as honorary skiagraphist.2 This early term for radiographer is derived from the ancient Greek skia (shadow) and grapho (writing)—particularly apt in the specialty’s early days, due to the blurriness of the images. By 1911, Hewlett was officially announced as skiagraphist at St Vincent’s Hospital, and at the Children’s in 1912, all the while operating his own radiology clinic in Collins Street. He served at the Children’s for 38 years, holding the roles of honorary physician, surgeon and radiologist.
Like his mentor Snowball in paediatrics, Hewlett at the Children’s Hospital laid the foundations for the development of radiography in Victoria and beyond. This was recognised on the international stage when he was honoured as a pioneer radiologist by the Antoine Béclère Centre in Paris.3
Professor Patricia Desmond
1 Royal Children’s Hospital. Address given by Sir Clive Fitts at the 99th annual general meeting held on 23rd September, 1969, p. 5. 1978.0103.00035, University of Melbourne Archives.
2 P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, p. 54.
3 Malcolm McKeown, ‘Hewlett, Herbert Maunsell (1872–1957)’, Australian dictionary of biography, vol. 9, Melbourne University Press, 1983.

-
Rebuffed by the Children’s
Grace ‘Clara’ Stone (1860–1957) was one of the first women medical graduates of the University of Melbourne, graduating with honours in 1891. She and her counterparts had publicly challenged the university hierarchy, compelling their enrolment into medicine—then still barred to women. Despite excelling in their studies, these pioneers met much opposition throughout their education and employment. Hospitals were unashamedly unaccepting of medical women, and even the few that did employ them still favoured male doctors.
In her early career, Clara assisted Dr John Singleton in Collingwood in providing free medical care to women and children of low socio-economic backgrounds. She also offered workplace health checks for women in local factories and school health checks for children.
In 1895 Clara, her sister Constance, and Melbourne’s handful of women medical graduates established the Victorian Medical Women’s Society (VMWS). Clara and the VMWS saw a gaping need to break down the barriers to women and children receiving timely and affordable health care, tackle some of the social determinants of health, and provide culturally appropriate medical care—in particular family planning, sexual health care, and maternal and child health advice. They also worked with women’s rights activists Vida Goldstein and Annie Bear-Crawford in campaigns to abolish child prostitution, raise the age of sexual consent, and improve working conditions for women.
Many of these objectives were achieved when Clara, Constance and their cousin Mary founded the first hospital for women, run by women. Opening in 1896 as a modest outpatient clinic at the Welsh Church in La Trobe Street, it was immediately overwhelmed by demand and moved to a larger site, becoming the Queen Victoria Hospital. Here, many of Australia’s pioneering medical women would receive training, undertake research, and develop public health programs.
Although Clara, the first woman doctor to seek a position at the Children’s Hospital, was unsuccessful in her application, she and her fellow medical women challenged the status quo and saw to the gradual acceptance of women in the medical profession. They were instrumental in making the education and employment of women in medicine inclusive and fair, and provided a voice for the needs of women and children in society.
Dr Anne Stanaway

-
The hospital’s first woman doctor
Dr Ethel Mary Vaughan Cowan (1868–1943) was the first female doctor employed at the Children’s Hospital, paving the way for innumerable women.
After undertaking nursing studies at Ballarat Hospital, Cowan graduated from the University of Melbourne in 1897 with a Bachelor of Medicine, only six years after the first female medical graduate. She was one of only two women in her graduating class, and subsequently also graduated with a Bachelor of Surgery in 1898.
Dr Cowan faced rejection at her first few attempts at medical employment, including her application to return to Ballarat Hospital. Her application to work as an assistant medical officer at the Women’s Hospital was accompanied by the ‘most flattering testimonials’, and her talents were described by the president of the hospital. However, a committee composed of women almost unanimously elected one of the two male applicants. This prompted a scathing article in Melbourne Punch:
Oh! woman, in your hour of ease
You may abuse us as you please;
When pain and anguish wring your brow
You want a male M.D., we vow.1
In 1898, Dr Cowan was offered a one-month trial in the outpatients’ department of the Children’s Hospital, without pay. Following her success in this role, she was offered a landmark appointment: an 18-month residency. This opportunity cemented Mary Cowan as the first female resident doctor at the Children’s Hospital, and one of the first in Victoria. Sir Charles Ryan (a member of the honorary medical staff) said: ‘I have formed a high opinion of her ability, and take pleasure in recommending her to any institution requiring the services of a well-qualified Resident Officer.’
Dr Cowan resigned the following year, and sailed to London on the steamer Yarrawonga as the ship’s registered doctor. This was an extraordinary occurrence—a female doctor from Melbourne did not travel again as a ship’s doctor for another 27 years. On returning to Melbourne in 1902, Dr Cowan was appointed honorary physician to the outpatients at the Queen Victoria Hospital (which had nine other female honorary medical staff), but resigned later that year. In 1904 she married William Stanley John Eaves and had two children, almost certainly signalling the end of her career, but leaving an undeniable legacy.
Dr Sarah McNab
- Melbourne Punch, 20 January 1898, p. 3.

-
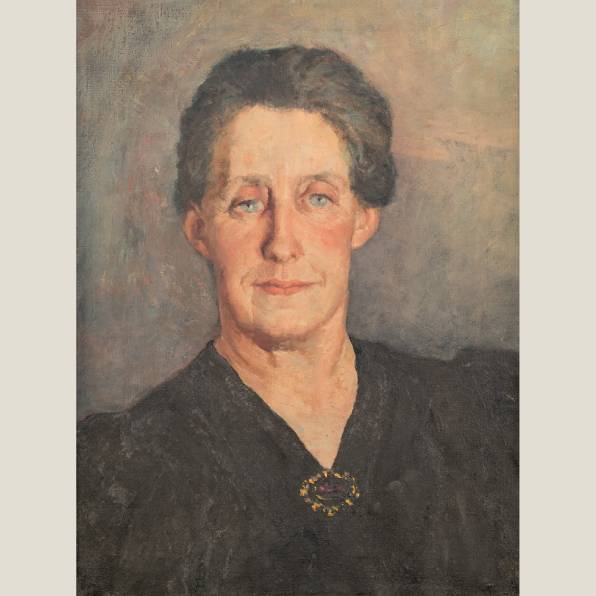
A reforming leader
Ella Latham (1878–1964) began her association with the Children’s Hospital as president of the newly formed Hawthorn Auxiliary in 1923. This preceded her appointment to the hospital’s committee of management in 1926, and she eventually became its longest-serving president, from 1933 to 1954.
Eleanor (Ella) May Tobin was born in the Melbourne suburb of Northcote. Her parents, both teachers, encouraged her further education, and she completed a Bachelor of Arts at the University of Melbourne in 1904. In 1907 she married John Latham, whose career in law and politics gained him a knighthood in 1935.
In 1932 Ella Latham established a rehabilitation centre in the Frankston Orthopaedic Section and formed the Victorian Society for Crippled Children in 1935. Despite renovations in train at the Carlton site, the committee of management decided in 1937 that the hospital should be relocated. But it was not until 1947 that the Minister for Health, persuaded by Latham and hospital manager Howard Barrett, offered the site on the corner of Flemington Road and Gatehouse Street, Parkville. Nine years later construction began, with staff and patients moving in six years after that.
Latham expanded the hospital’s medical appointment board in 1941 to include two representatives from the university, and instigated reform of the traditional honorary medical system. The first permanent medical director, Dr Vernon Collins, was appointed in 1948.
Bequests from the Burton family enabled a clinical research unit to be established, with Dr Howard Williams appointed as director in 1948. In 1951 the university recognised the unit for postgraduate Master of Science students to undertake further work.
Under Latham’s leadership and presidency, improvements were made to the hospital’s standards of care, administrative structure and funding. It has been said that she led the transition from 19th-century charitable hospital to modern teaching hospital, while coping with the additional difficulties of economic depression and a world war.
Lady Ella Latham was awarded a CBE in 1954 in recognition of her contribution to the public health care of children. The new lecture theatre in 1963 was named in her honour, as is the one in the new Parkville hospital.
Suzanne Scott
References: M McInness, Caring for our children: The history of nursing at the Royal Children’s Hospital, Melbourne, Melbourne: Australian Scholarly Publishing, 2006; P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999; L Gardiner, Royal Children’s Hospital Melbourne 1870–1970, Melbourne: Malcolm Printing, 1970.

-
A surgeon with an eye to the future
Sir William Upjohn (1888–1979) is one of the great figures in the history of the Royal Melbourne Hospital and the University of Melbourne. So it is ironic that in his later years he boasted that his entry to heaven was assured by the fact that he had ‘got Jean Macnamara and Kate Campbell on at the Children’s’.1 Despite having accepted women residents during World War I, the Children’s Hospital denied women places in the early 1920s. Upjohn’s representations to the hospital’s board resulted in their appointments, thus leading Campbell to a career in paediatrics, where she pioneered the field of neonatal medicine, and Macnamara to numerous important contributions, including revolutionising the care of children with poliomyelitis.
Upjohn graduated from the University of Melbourne MBBS in 1910, MD in 1912 and MS in 1913. During World War I he served in the medical corps at Gallipoli and on the Western Front, and was twice mentioned in dispatches. On return to Melbourne he was appointed as surgeon to outpatients at both the Melbourne and Children’s hospitals. He resigned from the Children’s in 1927 when he was promoted to inpatient surgeon at the Melbourne. He was one of three contemporaries who dominated surgery at the Melbourne Hospital for the next 20 years, the other two being Sir Alan Newton and Sir Victor Hurley.
Upjohn was one of the founding fellows of the Royal Australasian College of Surgeons. He held many prominent positions in medical, surgical and educational bodies, most notably as president of the Royal Melbourne Hospital (1960–68) and chancellor of the University of Melbourne (1966–67). He was knighted in 1958. His name is remembered by the university with the award of the Upjohn Medal for contributions to medicine in Australia, awarded every five years.
Though conservative in dress and mode of transport (driving a black Rolls Royce for 50 years),2 Upjohn was progressive in his views, predicting the end of the honorary system and, so many years earlier, advocating the cause of two young women doctors at the Children’s Hospital.
Professor Richard Larkins AC
1 Quoted in J McCalman, ‘Campbell, Dame Kate Isobel (1899–1986)’, Australian dictionary of biography, vol. 17, Melbourne University Press, 2007. 2 JV Hurley, ‘Upjohn, Sir William George Dismore (1888–1979)’, Australian dictionary of biography, vol. 16, Melbourne University Press,2002.
-
Catalyst for a statewide health service
Although Dr Vera Scantlebury Brown died 75 years ago, her legacy to Victoria remains a vibrant part of our state’s health system. In 1926 she was appointed as the inaugural director of infant welfare in Victoria, thus also becoming the first woman to head a state government department. She began with a small number of baby health centres run by devoted volunteers, and gradually transformed the service into a professional, statewide system.
Vera Scantlebury (1889–1946) graduated from the University of Melbourne’s medical school in April 1914 and, as the Great War rolled on, rose to become senior resident at the Children’s Hospital. Only the exigencies of wartime overcame the hospital board’s strong resistance to appointing women. But Vera wanted to contribute more directly to the war effort, and in late 1916 accepted a position as assistant surgeon at London’s Endell Street Military Hospital, known as the ‘suffragette’ hospital. There she joined 180 women—doctors, physicians, nurses, voluntary aid detachments and orderlies—and performed surgery in the operating theatre from May 1917 to January 1919. Between 1915 and 1919 the hospital treated more than 26,000 wounded, injured and sick soldiers, but Vera believed that her wartime work would count for little at home.
Vera returned to Melbourne in 1919, desiring to rejoin the Children’s Hospital as an honorary—the gateway to developing a paediatric practice. In 1924 she travelled to New Zealand, Canada, New York and Chicago to study child health, and completed her MD. But she was stymied in successive attempts at obtaining an honorary post and finally reconciled herself to a career in public health. Between 1926 and 1946 Vera led the development of 316 baby health centres, subsidies for 85 free kindergartens and 18 mobile units, and a correspondence school scheme for isolated country families. Today, Victoria enjoys a world-renowned, universal and free maternal and child health service, and Dr Vera Scantlebury Brown lies at the heart of it.1
Dr Heather Sheard
- References: H Sheard & R Lee, Women to the front: The extraordinary Australian women doctors of the Great War, Melbourne: Penguin Random House, 2019, pp. 142–8; H Sheard, A heart undivided: The life of Dr Vera Scantlebury Brown, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, 2016, p. 184.
-
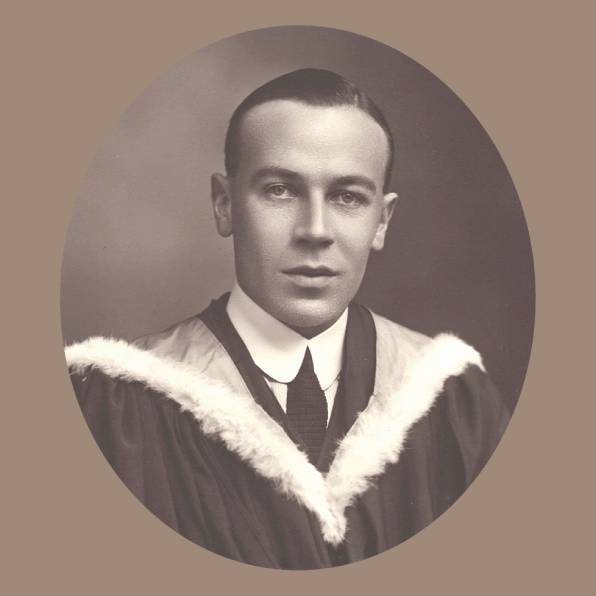
A lifetime of service
I am very pleased to write about my father’s numerous roles at the Royal Children’s Hospital. Dad was proud of his long association with RCH, which went back to his time as a resident medical officer in 1922.
Dr Robert Southby OBE, OStJ, MD, BS, FRACP, FACST(Hon) (1897–1991) was assistant pathologist in 1923, medical superintendent 1924–25, clinical assistant 1926, honorary attending medical officer to the venereal diseases clinic (treating infections contracted during childbirth) 1926–33, and honorary attending physician 1934–57. From 1950 he was the first lecturer in paediatrics at the University of Melbourne (part-time). After retiring from private practice he was consultant paediatrician to the Department of Health, Victoria.
Throughout his career my father was active in numerous organisations, including the BMA/AMA, Medical Society of Victoria, Medical Board of Victoria, Paediatric Society of Victoria and Australian Paediatric Association.
As a medical student he served in the Melbourne University Rifles, where he became a lifelong friend of Robert Menzies. Many years later, when attending meetings in Canberra, he and the prime minister often enjoyed dinner together.
My parents spent countless hours planting bushes and flowers and enjoying the peace and quiet of their riverside block at Kangaroo Ground. In the Medical Journal of Australia Dad once emphasised the significance of the ‘bush’ in providing respite from a busy professional life. He served as a district surgeon in the St John Ambulance Brigade in Victoria, and I followed him into that worthy organisation. After retiring from the Department of Health, Dad ran the first survey of abused children seen in the Casualty Department of RCH. It led to the implementation of the formal reporting system by the Victorian government. Dad always continued to write; I think his last piece was ‘Recollections of a geriatric paediatrician’.
I know that I am biased, but I believe that my father demonstrated many of the essential virtues and characteristics of a good physician: a strong intellect, compassion, commitment to his patients and their families, and a belief in service for the betterment of society. I am sure he would be delighted to see how RCH has continued to grow and develop over the years.
Professor Emeritus Dr Richard F Southby KStJ
-
Making a difference for children with disabilities
Annie Jean Macnamara (known as Jean, 1899-1968) grew up during World War I and resolved that she ‘wanted to be of use in the world’. Over her life, she realised this vision by making substantial contributions as a scientist, clinician and teacher.
As one of the earliest female doctors at the Children’s Hospital, her appointment in 1923 coincided with a poliomyelitis epidemic. In collaboration with Macfarlane Burnet, she discovered that there was more than one strain of polio virus, an early step towards the development of a vaccine. But her efforts were not confined to the laboratory; she was responsible for the development of an efficient and comprehensive system of care for children with poliomyelitis. In 1931 she was awarded a Rockefeller Fellowship, and visited Britain and the United States, where she furthered her skills in physical treatment, adapting splints and devices to immobilise, protect and allow rehabilitation of paralysed limbs. She applied these skills not only to children with poliomyelitis, but also to those with other conditions, including cerebral palsy. While in the United States she acquired Australia’s first artificial respirator.
For a long period (1928-51) Jean Macnamara was honorary medical officer to the Yooralla Hospital School for Crippled Children, the organisation now known as Yooralla. She also introduced a range of programs to meet the diverse needs of children with disabilities and their families. In 1938 she organised a daily program at the Children’s Hospital, which included transport and provision of a midday meal. For other children, she understood that community-based services would be preferable, and pioneered the establishment of regional services.
Often working long hours and without fees, she treated children with compassion and skill, listened to and counselled their families, and valued a team approach, consulting with splint-makers and physiotherapists. For her outstanding contribution to the care of polio sufferers, she was made a Dame Commander of the Order of the British Empire (DBE) in 1935. In 1966 she became the first woman to be awarded an honorary Doctorate of Laws by the University of Melbourne. Dr Jean Macnamara truly made a difference. Her legacy has paved the way for the care of children with disabilities today.1
Professor Dinah Reddihough AO
1 References: P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 196-7; K Bond, ‘Dame Annie Jean Macnamara DBE: A determined clinician’, in J Healy (ed.), Strength of mind: 125 years of women in medicine, Medical History Museum, University of Melbourne, 2013, p. 70; AG Smith, ‘Macnamara, Dame Annie Jean (1899–1968)’, Australian dictionary of biography, vol. 10, Melbourne University Press, 1986.
-
A physician and radical reformer
Together with Lady Latham, Vernon Collins was the prime mover in revolutionary changes that transformed the former charity hospital into a great teaching and research institution providing scientific and humane patient care. These radical innovations led to practices that now seem commonplace.
Vernon (1909–1978) attended Horsham High School, where the perceptive headmaster persuaded him to become a doctor—an unusual career choice for a western Victorian farmer’s son at that time. After graduation in 1933 and years as a resident, Vernon became medical superintendent (equivalent today to chief resident) at the Children’s Hospital in Carlton (1937–39). Dismayed by the nurses’ poor health and diet, he introduced improvements to their hospital food—an early hint of the future innovator.
Lady Latham recognised the need for a senior paediatrician to be in charge at the Children’s, and in 1949 Vernon was appointed as its first medical director. In 1959 he became inaugural Stevenson Professor in Child Health (the title changed in 1965 to Stevenson Professor of Paediatrics), and continued in that role despite progressive Parkinson’s disease in his final years, retiring in 1974.
Vernon’s major achievement was replacing the unpaid honorary consultant system with salaried senior medical staff. This allowed young doctors to earn a living as paediatricians, and ensured a more consistent consultant presence at the hospital, including salaried full-time department heads.
Among other pioneering initiatives, he replaced the very restricted inpatient visiting times with more liberal arrangements, directed that the parents of deceased children be interviewed by medical staff and their agreement obtained before any autopsy, and reorganised the outpatient clinics in order to ‘humanise’ the patient experience there. While implementing these and other reforms, Vernon continued his commitment to patient care and the teaching of medical students and paediatric trainees. He strongly advocated for and supported research, including unpopular projects that he saw as important. He identified and supported promising young doctors in securing further training and employment.
Vernon Collins shared his broad vision of paediatrics and of the needs of children and families, including the psycho-social aspects. He foresaw the new challenges to paediatric practice, as infections and other childhood diseases diminished.1
Dr Kevin Collins
1 References: H Williams, ‘Vernon Leslie Collins: An appreciation’, Australian Paediatric Journal, vol. 10, 1974, pp. 258–61; P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 310–13, 350–1; H Williams & AL Williams, ‘Obituary’, Australian Paediatric Journal, vol. 14, 1978, pp. 128–30.

-
A long life of service and generosity
One of the goals that guided my grandmother was to be useful to others.
Dame Elisabeth Murdoch (1909–2012)—Granny to me—enjoyed a remarkable and long life. Her generosity of spirit benefited many, but especially the children of Victoria. She spent some 85 of her 103 years helping the Royal Children’s Hospital and our sick children. This association began when, as a high school student at Woodend, she won the prize for knitting the most woollen singlets for needy babies; her reward was a tour of the hospital’s wards. The bond she forged that day with our sickest and most vulnerable young people continued thereafter, and she spoke often of the experience.
Always one to get involved, in 1933, aged 24, she joined the hospital’s management committee, eventually serving as president from 1954 to 1965. Add to that her involvement with the Royal Children’s Hospital Research Foundation, and her role as patron of the auxiliaries. I know she would have been delighted to have the Dame Elisabeth Murdoch Nursing Scholarship named in her honour, as she so admired and respected the nurses, doctors and staff. And significantly in 1986 she established, with Professor David Danks, the Murdoch Children’s Research Institute, which has grown from three researchers into a globally significant leader in childhood medical research, with more than 1,200 researchers.
Her lifelong determination to improve children’s health shaped her formidable reputation and forged a legacy to last the ages. She was heavily involved in the Good Friday Appeal, which her husband, my grandfather Sir Keith Murdoch, helped establish, and was known in her younger years to be wheeled down Mornington’s streets in a wheelbarrow to raise funds. The Good Friday Appeal has raised $399 million for the hospital, and in 2021 celebrated its 90th year.
Ultimately, Granny believed that our children hold the keys to a brighter future, and she was instrumental in shaping the Royal Children’s Hospital into what we know today: a world-class children’s hospital.
Penny Fowler

-
A true leader in child health
Howard Ernest Williams AO, MBBS, MD, FRACP (1910–1999) played a pivotal role in the evolution of clinical research at the Royal Children’s Hospital. After holding resident medical officer and registrar positions there in 1936–38, he was appointed medical superintendent (1939–41). Following war service with the RAAF, he became the hospital’s first full-time director of clinical research. Lacking formal training in research, he took up a Nuffield Fellowship to train with Sir James Spence in Newcastle, UK. This experience of social paediatrics later influenced paediatric research at RCH.
As the first paediatric thoracic physician in Australia, and one of the first in the world, Williams held many influential local, national and international appointments, including president of the Australian College of Paediatrics and president of the Thoracic Society of Australia. His broad-ranging research included pyloric stenosis (a blockage of the small intestine), bronchiectasis (an inflammatory lung condition) and asthma. He appointed Charlotte Anderson as the first research-funded RCH medical officer. Howard became known as ‘the professor maker’, with colleagues including Professors Anderson, Bill McDonald, Graham Mortimer, Ivo Carre, Peter Phelan and Louis Landau. Ironically, his own University of Melbourne professorial associate appointment came after he ceased clinical practice.
Later he was drawn more towards social medicine, including breast feeding, preventing diarrhoea, and the association of accidental poisoning with poor housing. With his research fellow Allan Carmichael (another of his ‘professors’), he embarked on ‘The Brunswick Study’, a longitudinal study of 224 children up to four years of age, which showed a high incidence of behavioural disturbance (22%) contrasting with low incidence of serious organic morbidity (4%). These controversial findings helped stimulate a new stream of community-based child health care. This ‘fingerprint’ remains on the RCH.1
Howard Williams was the first RCH paediatrician employed to do research, and the first to appoint an RCH full-time research medical officer. He questioned the dominance of organic medicine, and forged a path in community-based child health. His huge contribution is recognised by the Howard Williams Medal, awarded annually by the Royal Australasian College of Physicians.
Professor Graeme Barnes AO
1 Peter Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 321–7.
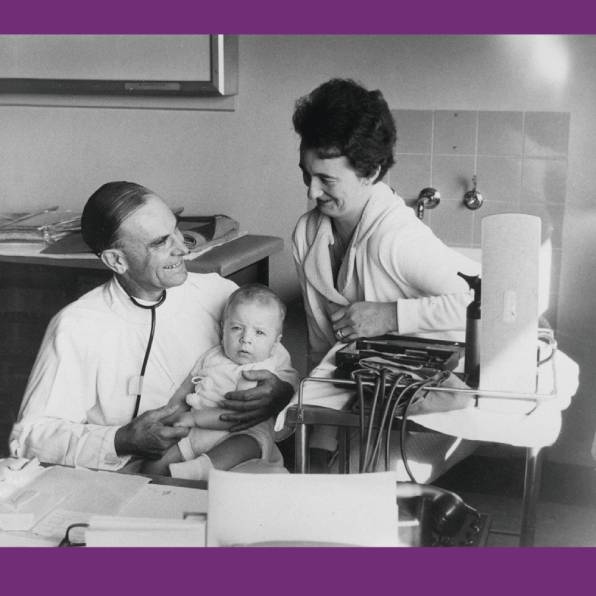
-
A paediatrician at the vanguard
Dr Elizabeth Kathleen Turner (1914–1999) worked as a paediatrician at the Children’s Hospital from 1942 to 1980. When she became medical superintendent (1944–46), The Argus reported that she would be the first woman to ‘hold such a position’ at the hospital. Her career was spent at the vanguard of paediatric medicine.
In 1944 Turner, having graduated MBBS from the University of Melbourne just four years earlier, visited the enormous US military camp in Royal Park. She was on a mission: it was World War II and the Americans had precious supplies of a new drug, penicillin. Turner needed it as a life-saving treatment for one of her patients in the Children’s Hospital, eight-year-old Allan Goates, who had osteomyelitis of the humerus (infection of a bone in the arm). She got the drug and, after intensive intravenous treatment and surgery, Allan recovered.
In 1951 Turner introduced to Melbourne the concept of sick babies having their mothers with them in hospital, which she had observed in England. Today, it is unimaginable for a mother to not be permitted to care for her infant in hospital.
Turner’s stellar career included numerous publications in the Medical Journal of Australia and references in daily newspapers. Her research covered topics such as neonatal meningitis, Aicardi syndrome (a rare congenital disorder of the brain and eyes), A B O blood groups and foetal erythroblastosis (incompatibility in blood type between mother and child, causing anaemia), foetal alcohol syndrome, the deaf child, thalassaemias (a type of inherited blood disorder), Ehlers-Danlos syndrome, and kernicterus (a bilirubin-induced brain dysfunction). She was an important advocate for paediatric health care in Victoria.
As president of the Victorian Medical Women’s Society in 1983, Turner acknowledged the inner strength that women needed to become doctors, recalling that in 1941 the Alfred Hospital had approved her internship on the proviso that ‘you will have to agree to one year of single blessedness’.
Each year the Medical Staff Association of the Royal Children’s Hospital reflects on Dr Elizabeth Turner’s extraordinary life by awarding a medal in her name, to a senior staff member in recognition of years of service and contribution to patient care.
Associate Professor Susan M Carden
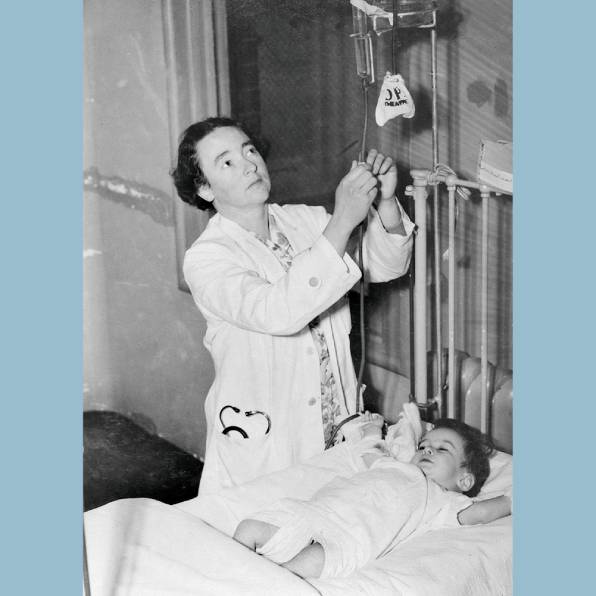
-
A humane doctor, who put research first—and patients equal first
Few Australian doctors have contributed to the daily lives of people experiencing the chronic and debilitating conditions coeliac disease and cystic fibrosis as did Melbourne–born and educated paediatric gastroenterologist Charlotte (or, as she preferred, ‘Charlo’) Anderson (1915–2002).
While working in England in the early 1950s, Anderson was part of the team that identified gluten as the protein in wheat responsible for coeliac disease, wherein the small intestine cannot digest and absorb certain types of food. The resulting failure to thrive, intestinal pain, bloating and diarrhoea affect an estimated one in 70 people in Australia. Following publication of this finding, Anderson was offered a senior clinical research role with the Children’s Hospital in Melbourne (1962–68), where she went on to establish the gastroenterology research unit, introduced gluten-free diets for coeliac patients, and worked with the food industry to produce gluten-free foods.
It was a homecoming for Anderson in several senses: a return not only to the city of her birth, family and education—which included a Master of Science degree gained while undertaking laboratory research at the Baker Medical Research Institute and a medical degree at the University of Melbourne—but also to the Children’s, where she had worked before going overseas. Her focus then had been cystic fibrosis (a condition that combines poor digestion and malabsorption of food with chest disease) and its differentiation from coeliac disease in infancy. She continued this work in London and Birmingham.1
In 1968, on her appointment as professor of paediatrics and child health at the University of Birmingham, she became the first female professor of paediatrics in either Australia or the United Kingdom. She served in the position for 12 years, assisting and supporting innumerable patients and their families, co-authoring some 60 academic papers, and in the 1970s co-editing the standard reference text Paediatric gastroenterology and an accessible text for health care professionals, Cystic fibrosis: Manual of diagnosis and management. She was active in professional affairs, and was once described as ‘arguably the “Mother of Paediatric Gastroenterology”’.2
Dr Ann Westmore AM
1 ‘Charlotte Anderson’, in R Andrew & A Barnett (eds), In their day: Memoirs of alumni; The Baker Medical Research Institute, Melbourne: Hyland House, 1992, pp. 19–24; N Allen, ‘A pioneer of paediatric gastroenterology: The career of an Australian woman scientist’, Historical Records of Australian Science, vol. 11, no. 1, June 1996, pp. 35–50.
2 EV O’Loughlin & DJS Cameron, ‘History of paediatric gastroenterology in Australia’, Journal of Paediatrics and Child Health, vol. 56, no. 11, November 2020, pp. 1669–73.
-
An outstanding paediatric surgeon
Peter Jones (1922–1995) was a surgeon ahead of his time, being the first general surgeon in Australia to obtain the FRACS in paediatric surgery. In 1953 he was appointed as a staff surgeon in the General Surgery Department of the Royal Children’s Hospital, where Russell Howard was the chief, a direct result of Professor Vernon Collins’ initiative to establish staff specialists in both medicine and surgery. Before that (and everywhere else in the world), consultant physicians and surgeons were honorary, and needed a private practice in adult medicine to survive financially.
Peter had a flair for seeing the opportunities of full-time work at RCH. For the hospital’s centenary in 1970 he edited the world’s first textbook on the new subspecialty of paediatric surgery, which became a great success and is now in its seventh edition. He was also instrumental in establishing the combined therapy clinic, to pool knowledge on treating cancers, especially solid tumours that needed the new anti-cancer drugs as well as surgery and/or radiotherapy. By 1976 he and Dr Peter Campbell were able to edit the first textbook on paediatric solid tumours, with contributions from staff across the hospital through the combined therapy clinic records.
Before Peter obtained the FRACS in paediatric surgery he had an English fellowship in general surgery, and a Master of Surgery on torticollis (a neck injury once common after breech delivery). As paediatric surgery advanced, subspecialisation became important, and Peter developed the hepatobiliary unit (liver, bile ducts and gallbladder) in general surgery, along with Russell Howard and Nate Myers in thoracic surgery and Douglas Stephens and Durham Smith in urology.
Peter was recognised internationally by honorary fellowships of the American College of Surgeons and the American Academy of Pediatrics, and beyond paediatrics he was a councillor in the Australasian College of Surgeons for eight years, as well as president of the Australian Association of Surgeons (1983–86).
Outside medicine Peter was a legendary raconteur and expert on heraldry (he helped design the RCH’s coat of arms, as discussed on page 34). At the end he was working on a thesis on Dr Roderigo Lopez, Queen Elizabeth I’s personal physician, who was executed for treason.
Professor John Hutson AO
-
Understanding grief, bereavement, and the child’s inner world
In October 1956 a young English doctor gave a talk at the Paediatric Society of Victoria on ‘Preparation of children for tonsillectomy’. Dr Jones was eight months pregnant, not yet working at the Royal Children’s Hospital, and subsequently published her research emphasising the need for psychological preparation of the pre-operative child in the Medical Journal of Australia, where she thanked Vernon Collins, who had been busy initiating the controversial psychosocial intervention of liberalising restrictions on parental visiting.1
Eighteen years later (now with six children and employed as a child psychiatrist), Dr H Julie Jones (1926–2017) joined a small group of female consultants, and went on to make a deep impression on the RCH. She published with some of the most respected members of staff (Henry Ekert, Dinah Reddihough, Louis Landau and Kester Brown), focusing on the child’s experience of hospitalisation, bereavement, grief, the dying child, and the importance of funerals in the mourning process. She taught her colleagues to regard their small patients as interesting, sentient beings with an inner world.
Dr Jones articulated the need for grief, loss and bereavement to be raised in the hospital’s hierarchy of practice, believing that children’s emotional experiences should be placed at the centre of all encounters; in her shy English way, she argued for this boldly. With the Social Work Department, she initiated the Bereavement Group, offered to all the hospital’s bereaved parents. This was a powerful systemic change for the hospital: to extend its reach to support parents long after their child had died. She worked closely with allied health staff and advocated for them fiercely, also supporting coroner’s court staff dealing with traumatic deaths. Following the 1983 Ash Wednesday bushfires, Dr Jones took up both a clinical and public role in explaining children’s responses to this environmental trauma. Her 1990 paper on ‘Children’s reactions to the murder of their mother by their father’ foreshadowed contemporary awareness of the serious effects of family violence on children.
At Julie’s funeral in 2017, 60 years after her Paediatric Society presentation, at least half of the standing-room-only congregation were RCH alumni or staff.
Penelope Jones and Sarah J Jones
- References: HJ Jones, ‘Preparation of children for tonsillectomy’, Medical Journal of Australia, vol. 1, 1958, pp. 31; IH Jurk, H Ekert & HJ Jones, ‘Family responses and mechanisms of adjustment following death of children with cancer’, Australian Paediatric Journal, vol. 17, 1981, pp. 85–8; E Berah, HJ Jones & P Valent, ‘The experience of a mental health team involved in the early phase of a disaster’, Australian and New Zealand Journal of Psychiatry, vol. 18, 1984, pp. 354–8.

-
The father of clinical genetics in Australia
Today it is hard to believe that in the 1960s and 1970s the international meetings of researchers in human genetics were attended by just a few hundred doctors and scientists. In those years the most respected clinician was Victor McKusick, from Johns Hopkins in the USA, around whom gathered a small group of ‘gurus’. David Danks was already regarded as an outstanding intellect in clinical genetics, a field that hardly existed anywhere apart from Johns Hopkins, Harvard, London, Paris—and Melbourne.
David Danks (1931–2003) had qualified in medicine at Melbourne in 1954, and was ‘spotted’ for his ability and hard work by Howard Williams, director of RCH Clinical Research Unit, where he trained. Unusually for the time, he researched the basic causes of diseases, and recognised the significance of genetics to paediatrics. He studied at Great Ormond Street and at Johns Hopkins with McKusick. The Danks family was long part of Melbourne’s commercial scene, and David was one of the few doctors with strong links to ‘Melbourne royalty’. Many of these already supported the RCH, none more than Dame Elisabeth Murdoch. When David gave up his role as Stevenson Professor of Paediatrics in 1980 he approached Dame Elisabeth and her friends (and the NHMRC) for support for his work through the Birth Defects Research Institute, which became the Murdoch Institute for Research into Birth Defects.
David built a strong group of clinicians, including John Rogers and Agnes Bankier. Most clinical geneticists in Australia and New Zealand were trained by David and John. When David retired in 1995 the Murdoch Children’s Research Institute was internationally renowned for its clinical and research excellence, with a focus on ‘traditional’ genetics: single-gene disorders and chromosomal defects. The future of genetics, however, lay elsewhere. The human genome project, the interaction between genetics and environment, and the role of genetics in cancer, heart disease and mental illness meant that genetics must be understood by every doctor (and nurse), be shared with the community, and underpin paediatrics and public health. The Murdoch Children’s Research Institute is indeed David’s legacy, but I am not sure he would recognise it today. It has grown from about 150 staff in 1995 to 2,000 in 2021, and researches every aspect of infant, child and adolescent health.
Professor Bob Williamson AO
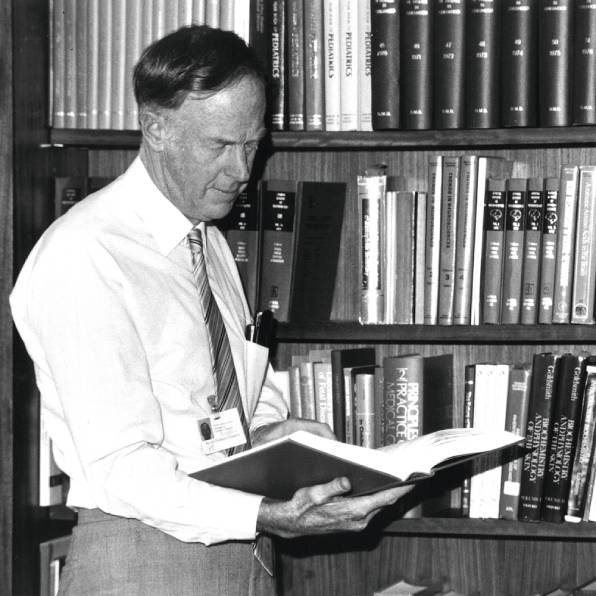
-
Ruth Bishop and the rotavirus story
As a bacteriologist in the laboratory of the Department of Gastroenterology at the Royal Children’s Hospital, Ruth Bishop was frustrated that she could not identify the pathogen responsible for more than 70 per cent of cases of childhood diarrhoea admitted to hospital. The development of a novel small-bowel biopsy capsule by the director of gastroenterology, Dr Rudge Townley, presented the opportunity to search for the elusive pathogen by using the new scanning electron microscope at the University of Melbourne. This collaboration, led by Ruth and involving RCH clinicians Geoff Davidson, Graeme Barnes and Don Cameron, and University of Melbourne scientists Ian Holmes and Brian Ruck, was responsible for the discovery of rotavirus and understanding the effects of this common pathogen that each year caused more than half a million deaths in children worldwide.1
Rotavirus vaccines have now been introduced in more than 110 nations, resulting in the prevention of death and hospitalisations due to gastroenteritis. But the work was not yet done. Ruth identified the neonatal rotavirus strain RV3, found in the stool of healthy babies in newborn nurseries in Melbourne and shown to be protective against severe rotavirus disease in the first three years of life.2 This novel rotavirus strain forms the basis of the RV3-BB vaccine, which protects against rotavirus disease from birth and has been licensed for global use.3
The prevention of rotavirus disease became Professor Ruth Bishop’s life’s work, and it has not gone unnoticed. For her services to medical research she was made an Officer of the Order of Australia (AO) in 1996 (raised to AC in 2019). She was inducted into the Victorian Honour Roll of Women in 2001, received the Prince Mahidol Award from the Thai royal family for outstanding achievements in public health in 2011, and in 2013 became the first woman to be awarded the Florey Medal. Ruth’s global contribution has been far reaching, as Bill Gates said in 2021: ‘Hearing about the number of children dying from rotavirus sparked a fire in us many years ago. Thanks to Ruth’s pioneering research and laser focus, her passion for a solution to this overlooked disease became ours.’
Professor Julie Bines
- RF Bishop et al., ‘Virus particles in epithelial cells of duodenal mucosa from children with acute non-bacterial gastroenteritis’, Lancet, vol. 2, no. 7841, 1973, pp. 1281–3.
- RF Bishop et al., ‘Clinical immunity after neonatal rotavirus infection: A prospective longitudinal study in young children’, New England Journal of Medicine, vol. 309, no. 2, 1983, pp. 72–6.
- JE Bines, … RF Bishop … et al., ‘Human neonatal rotavirus vaccine (RV3BB) to target rotavirus from birth’, New England Journal of Medicine, vol. 378, no. 8, 2018, pp. 719–30.
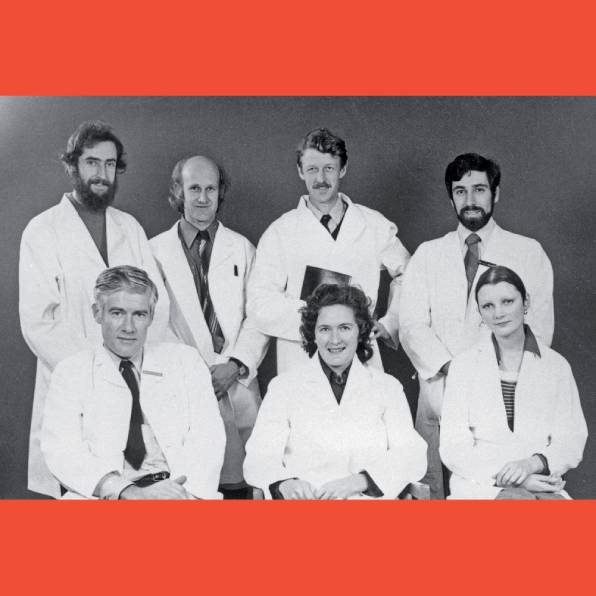
-
Child psychologist and advocate for peace and justice
Margot Prior Hansen (née Jones, 1937–2020) first trained as a pianist, oboist and music teacher at the University of Melbourne, where she met her first husband, Glen Prior. They married in 1958 and had three children: Yoni, David and Sian.
Following Glen’s untimely death in 1964, Margot returned to study, retraining as a psychologist. Her master’s and doctoral degrees examined a condition about which little was then known, autism, and she published the first Australian journal article on what is now known as autism spectrum disorder. She moved rapidly from a tutorship at Monash University to a lectureship at La Trobe University, where she apprenticed as a clinical psychologist while expanding her research interests in child developmental psychology to include attention deficit hyperactivity disorder, autism, dyslexia, child behaviour problems, developmental neuropsychology and temperament. She married John Hansen in 1969.
Margot became the first female professor of clinical psychology in Australia (1989). She designed and launched the Australian Temperament Study, the first longitudinal study of its kind—which continues to this day—and established the first clinical psychology doctoral program in the country. In 1994 she was appointed head of the Psychology Department at the Royal Children’s Hospital. There she founded the Learning Difficulties Centre and was a co-founder of the Victorian Parenting Centre (now the Parenting Research Centre).
Margot was a fierce public advocate for child welfare, peace and social justice. She co-founded Psychologists for Peace and the La Trobe Institute for Peace Research. From 2005 to 2007 she chaired the Social and Human Sciences Network for UNESCO, and travelled to India and Vietnam to train clinicians to support children with developmental difficulties.
Her ground-breaking work and advocacy were recognised with a Medal of the Order of Australia in 2004, and she was Victorian Senior Australian of the Year in 2006. A fellow of the Academy of the Social Sciences, Margot was awarded Doctor of Science (honoris causa) for her contributions to scientific and clinical knowledge, and received a Lifetime Achievement Award from the International Society for Autism Research. She retired from RCH in 2002 but continued her research, co-authoring many journal articles. Margot passed away in August 2020.
Dr Yoni Prior and Dr Sian Prior
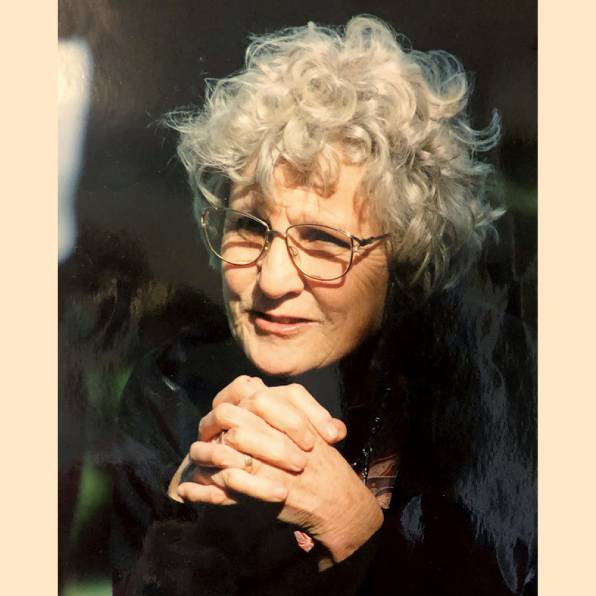
-
A versatile leader, with a talent for spotting talent
Peter Phelan BSc, MD, FRACP (b. 1939) came to the Royal Children’s Hospital as a paediatric registrar in 1965 and went on to have senior roles as a respiratory physician and researcher working in both clinical and epidemiological contexts. He became the foundation director of the Department of Thoracic Medicine, chairman of the Division of Specialist Medicine, Stevenson Professor and head of the Department of Paediatrics, and assistant dean for postgraduate studies, Faculty of Medicine, Dentistry and Health Sciences at the University of Melbourne. Peter served on the committee of management and boards of the hospital, the RCH Foundation and the Murdoch Children’s Research Institute. He also had many external roles, including as president of the Australian College of Paediatrics, chairman of the Committee of Presidents of Medical Colleges, chairman of the Specialist Accreditation Advisory Committee, Australian Medical Council, and member of the Metropolitan Hospitals Planning Board.
Peter was instrumental in helping establish paediatric respiratory medicine as a subspecialty in Australia. He understood the value of tight integration between the partners on the RCH campus and had influential roles in all areas, and a clear view that the success of the hospital and its partners lay in the quality of its people. He had the reputation for identifying those who he thought may be strong future leaders early in their careers (even as medical students) and then supporting them to achieve their best. Peter significantly built up the numbers of clinical trainees undertaking higher degrees and contributed to the strong academic reputation of RCH. He also had an important role in attracting overseas trainees to RCH, many of whom went on to have leadership roles in Australia or in their own countries.
Professor Peter Duhig Phelan AM was a great example of the strong relationship between the Faculty of Medicine, Dentistry and Health Sciences and the Royal Children’s Hospital over the 32 years he worked at the RCH.
Professor Mike South
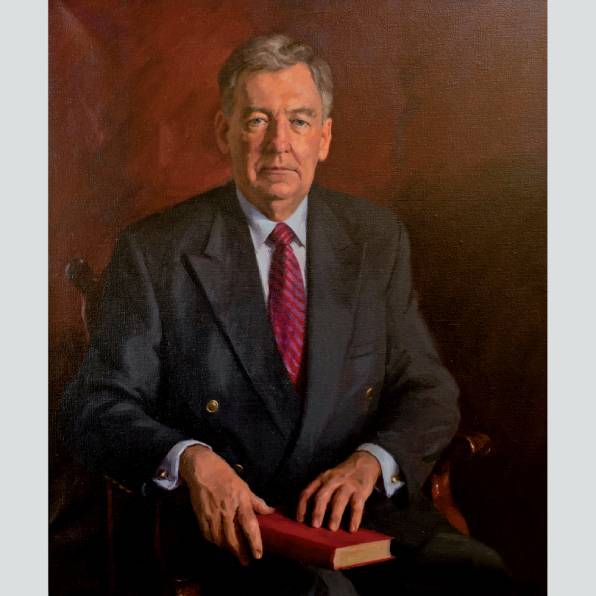
-
Paediatric intensive care
Dr Frank Shann, pictured here at the bedside of a seriously ill child, was the third director of the paediatric intensive care unit (PICU) at the Royal Children’s Hospital, from 1983 to 2005, and in 1995 became Australia’s first professor of critical care medicine, through the University of Melbourne.
Professor Shann’s research in paediatric intensive care contributed to several paradigm shifts in the practice of medicine. The scoring system he developed (called PIM) and his research comparing centralised and decentralised intensive care services have been used by policy makers to improve paediatric intensive care services in many countries. Shann also published Drug doses, used by tens of thousands of doctors and nurses around the world for three decades.
At the time of this photograph, a team of five ICU physicians worked at RCH:
Drs Frank Shann, James Tibballs, Warwick Butt, Rob Henning and Mike South. Tibballs was instrumental in developing the medical emergency team at RCH, and with Henning developed the home ventilation service, which now supports hundreds of children in the community. Henning ran the paediatric emergency transport service for 20 years, coordinating the care and transport of critically ill children from around Victoria. Associate Professor Warwick Butt was director of the PICU from 2011 to 2020. In the 1980s he had brought extracorporeal membrane oxygenation (ECMO) to RCH; ECMO is rightly credited with saving the lives of hundreds of children. Butt led the PICU when it moved to the new hospital in 2011 and established the model of care that we have today. He oversaw the expansion of the PICU team to 10 consultants, specialisation in cardiac and general intensive care, and the introduction of modern quality and safety mechanisms. Butt was succeeded as director in 2021 by Dr Thomas Rozen.
PICU works with every clinical department in the hospital, and has trained hundreds of doctors, nurses, allied health professionals and clinical technologists who have gone on to work in paediatric units across Australia, and throughout the world. Its world-class research program combines epidemiology, biosciences, clinical research, and technology. In the 1990s Professor Shann estimated that at least one in 80 Victorian children would spend time in PICU, and the figure is probably even higher today. PICU is a truly international unit that holds a special place in the hearts of the people of Victoria.
Professor Trevor Duke

-
To measure is to know’: From poliomyelitis to cerebral palsy
When you can measure what you are speaking about, and express it in numbers, you know something about it; but when you cannot measure it, when you cannot express it in numbers, your knowledge is of a meagre and unsatisfactory kind. (Lord Kelvin)
In the early 1990s, the Royal Children’s Hospital’s chief physiotherapist, Anne McCoy, and its senior orthopaedic surgeon, Malcolm Menelaus, had a vision of establishing a gait analysis laboratory at the hospital. McCoy embarked on a Churchill Fellowship to study gait laboratories in North America and Europe. Menelaus and Bob Dickens, the hospital’s director of orthopaedic surgery, formed a partnership with the Hugh Williamson Foundation to plan and fund the proposed laboratory. Orthopaedic surgeon Kerr Graham had been trained in gait analysis in North America and in 1994 was recruited to oversee the project. The Hugh Williamson Gait Laboratory at the RCH opened in 1995, and from the opening day was never short of patients!
In the early days, the majority of patients were children with cerebral palsy, spina bifida and other neuromuscular disorders. The laboratory revolutionised the management of children with gait problems and facilitated the introduction of botulinum toxin therapy, selective dorsal rhizotomy and single-event multilevel surgery (SEMLS). The laboratory has been an enabling technology for clinical trials and for the development of measurement tools that are now used internationally.1
Initially, there was a lack of expertise in both physiotherapy and biomedical engineering to staff the laboratory. That all changed when an increasing number of physiotherapists and mechanical engineers from the University of Melbourne enrolled for PhDs and became the home-grown experts to run the laboratory to the highest international standards. Since then, the laboratory has been awarded two National Health and Medical Research Council Centres of Research Excellence, and is recognised internationally for high standards in clinical service and innovative research.
In 2021, Kerr Graham was succeeded as director of the Hugh Williamson Gait Laboratory by Swiss-born orthopaedic surgeon Dr Erich Rutz, who had been a research fellow in the laboratory 10 years earlier.
Professor Kerr Graham
- HK Graham et al., ‘The functional mobility scale (FMS)’, Journal of Pediatric Orthopaedics, vol. 24, no. 5, 2004, pp. 514–20; R Baker …, HK Graham … et al., ‘The gait profile score and movement analysis profile’, Gait Posture, vol. 30, no. 3, 2009, pp. 265–9.

-
Pioneering paediatric chemotherapy in Australia
Born in Melbourne but educated in South Australia, John Haughton Colebatch(1909–2005) graduated in medicine in 1936, and after two years studied for postgraduate qualifications in England, where he also married. In 1939 he and his wife returned to Australia and John enlisted in the Australian Defence Forces, rising to the rank of major. At the end of the war he returned to Melbourne, and in 1946 was appointed as a paediatric consultant to the Children’s Hospital and Royal Women’s Hospital.
In 1948 in Boston Colebatch met with paediatric pathologist Dr Sidney Farber, regarded as the father of modern chemotherapy. After observing the results of aminopterin treatment of children with acute lymphoblastic leukaemia, Colebatch was the first in Australia to try to achieve prolonged remissions in such patients, and the first to commence clinical trails. He encountered much opposition, but eventually prevailed.
As the new chemotherapeutic agents became available, in the 1960s Colebatch recruited 12 paediatric institutions to participate in a clinical study of cyclical as compared to longitudinal maintenance treatment in leukaemia, which earned international acclaim. He practised and taught the discipline of adhering to protocol and achieving statistically significant results. He introduced the concept of a tumour board of specialists from all relevant disciplines to plan the treatment of children suffering from solid tumours, at a time when no one else did. In time this approach was accepted by adult oncologists, and is now almost universal.
To bring about these fundamental changes in attitudes to the treatment of cancer required wisdom, strength and an almost bulldog-like tenacity. John Colebatch had all of these, and for his contributions was made an Officer of the Order of Australia and received many other honours. His contribution to the remarkable progress in curing paediatric cancers cannot be overestimated; John Colebatch was truly the father of the modern treatment of cancer and leukaemias in Australia.
Professor Henry Ekert AM
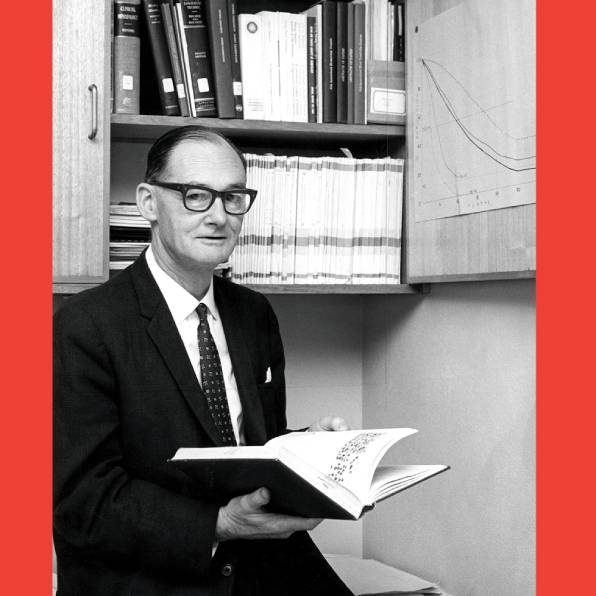
-
Cardiac transplant program
Heart transplantation for patients with heart disease emerged in 1967, with the first transplant performed by Dr Christiaan Barnard in South Africa. The patient lived for only 18 days, but several centres around the world attempted transplants in the following months. Most patients lived for only a few weeks or months, until the arrival of the immunosuppressant medication cyclosporin, which was first used for a transplant patient in 1980. Several units then started successful transplant programs, including Harefield Hospital in London (1980) led by Sir Magdi Yacoub, and St Vincent’s Hospital in Sydney (1983) led by Dr Victor Chang.
The Harefield program included children and was the model for the second program in Australia, which was set up in 1988 at the Royal Children’s Hospital in Melbourne. The chief executive officer of the hospital (Dr Barry Catchlove) and the director of cardiac surgery (Dr Roger Mee) were keen to start heart transplantation, and the appointment of a new director of cardiology in late 1987 provided the initiative. Dr James Wilkinson had worked with the Harefield team, caring for transplant patients, and used Harefield’s protocols to plan the program, which was approved by the Victorian government in September 1988. Professor Yacoub and his cardiologist, Dr Rosemary Radley Smith, were generous in their support to RCH at the time, helping ensure its program’s successful commencement. On 4 October 1988 the first transplant was performed, on 14-year-old Michael Sofoulis, who had a dilated cardiomyopathy. He survived for more than 23 years.
In 1991 the RCH transplant program was approved for national funding, becoming the first program to be given the status of ‘Nationally Funded Centre’. By mid-2015 a total of almost 300 patients had been assessed. Fourteen heart-lung or lung transplants were performed early in the program, but these were later taken over by the Alfred Hospital, which had the third Australian program, commencing in 1989.
The results have been encouraging, with patients operated on between 1996 and 2002 having a five-year survival rate of 86 per cent. Our team, which is still home to the National Paediatric Heart Transplant Centre, has recently performed its 200th heart transplant, and we have survivors who are more than 30 years post-transplant.
Professor James Wilkinson AM
![<strong><em>Ready to tackle the future: Michael [Sofoulis] and two of the men who helped give him a new life, cardiologist Jim Wilkinson and surgeon Roger Mee</em></strong>, in Sally Gibson, ‘A beat goes on’, Herald Sun, October 1989. David Johns (photographer) / Newspix.](https://museums.mdhs.unimelb.edu.au/__data/assets/image/0008/3945536/MHM_72-First-Transplant-RCH.jpg)
-
Complex surgery
A modern paediatric hospital is a collection of many people with many different skills—a team looking after sick children and their families.
One turning point at the Children’s Hospital in Melbourne was led by Professor Vernon Collins (later medical superintendent from 1948), who appointed staff to care only for children: physicians became paediatricians, and in the 1940s he appointed the respected general surgeon Russell Howard to operate on children only. Howard’s expertise resulted in Australia’s first successful repair of the birth defect oesophageal atresia, in the late 1940s. He became chief of surgery in 1952, in turn appointing other paediatric surgeons. Many advances were made possible by developments in anaesthesia and post-operative care. Gretta McClelland became director of anaesthesia in 1956 and John Stocks developed the intensive care unit in 1964. Complex and delicate operations on thoracic and abdominal problems could now be more safely and expeditiously performed.
Complex operations like the separation of conjoint twins need a large team of experts. The separation of two girls in 1988 (illustrated opposite) required neonatal physicians, radiologists, cardiac team and gastroenterologists. Another turning point towards paediatric specialists was in cardiac surgery. In the 1960s I was a trainee in the cardiac unit with George Westlake. He was a world-class surgeon and I am grateful for his teaching, but he was basically an adult surgeon. Progress accelerated with the appointment of Bill Braun from Birmingham and Roger Mee from New Zealand. For instance, transposition of the great vessels is a classic cause of ‘blue baby’. Bill Mustard in Toronto designed an operation to transfer the blood at atrial level, but the right ventricle was eventually too stressed to pump blood around the body. Roger Mee designed a ‘switch’ operation to restore the anatomy. Due to his skill and attention to detail, his first 50 operations on sick babies were performed without a single death—amazing!!
The RCH’s role in training paediatric surgeons means that its people now work all around Australia and the world. One area of particular interest is the South Pacific: Cook Islander Kiki Maoate trained at RCH, is now based in Christchurch, and is influential across the region. Finally, it is now recognised that actively involving the family is vital to the successful treatment of sick children.
Dr Alex Auldist AO
‘Surgeons separate twins in six hours’, Canberra Times, 20 October 1988. National Library of Australia.
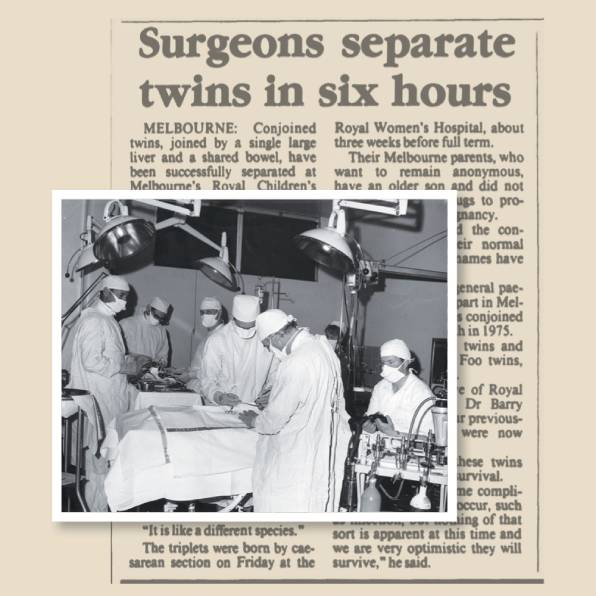
-
The miracle of vaccines
Infectious diseases have always been the major cause of sickness and death among children in Victoria, and they remain so today, causing one-quarter of children’s hospitalisations. However, their effects have been remarkably curbed by vaccines, and to a lesser extent by antibiotics. Put simply, immunisation of children is the greatest public health success story in recent human history, and Victorian children have been the beneficiaries since community immunisation began here in 1932.
Before the era of widespread immunisation, many children died from infections including pneumonia, meningitis, diarrhoea, measles and whooping cough. Management of these conditions was generally symptomatic and expectant, with very few effective therapies. Isolation of infected children was common. But between 1932 and 1970, vaccines against diphtheria, tetanus, whooping cough, measles and polio were introduced in Victoria. In 1930, the mortality rate of Australians aged under five years was 70 deaths per 1,000 live births. By 1970 it was 22 per 1,000. Although immunisation cannot claim all the credit, vaccines brought a huge benefit. The effect of the poliomyelitis vaccine is especially noteworthy. Polio was a devastating illness, and the Children’s Hospital dedicated tremendous resources to the care of afflicted children. Vaccines were introduced in 1956, and Australia’s last locally acquired case was recorded in 1972.
Vaccines for children and adolescents included rubella (introduced 1971), mumps (1981), hepatitis B (1983), meningitis (haemophilus 1992, meningococcus 2002, pneumococcus 2005), chickenpox (2001), rotavirus (2007), cervical cancer (2007), pandemic influenza (2009) and seasonal influenza (2010). In 2020, the child mortality rate was 4 per 1,000.
Of course, we do not have a vaccine for every infectious disease, and antibiotic treatment has also brought a remarkable reduction in death and disability. As discussed on pages 25 and 90, the first antibiotic given to a child at RCH was penicillin, administered in 1944. It remains useful against several infections, including pneumonia and sore throat, although the rising danger of resistance to antibiotics means that fewer conditions can be treated with penicillin today than in the 1940s.
Fast-forward to 2021, and the COVID-19 pandemic is a stark reminder of the ever-present threat of infectious diseases, but also of the astonishing power of immunisation.
Professor Andrew Steer

-
Paediatric nursing education
When the Melbourne Free Hospital for Sick Children opened in 1870, there was no organised general nursing training in Victoria; most skills were handed down from one nurse to another. In 1879 Mrs Bellaine, a graduate of Sydney’s Lucy Osburn nursing training school, which espoused the Nightingale principles, was appointed assistant matron to Mrs Sarah Bishop. Bellaine incorporated the Nightingale principles into the Free Hospital’s emerging training program, and by 1887 the hospital was officially recognised as a nursing training school.
After two years of lectures on anatomy, physiology and general nursing, a student would receive a certificate showing attendance. Evelyn Conyers (1870–1944) obtained her certificate in 1894 at the Children’s Hospital, and became a foundation member of the Nurses’ Registration Board and the Victorian Trained Nurses Association in 1901. Together with other members from the Melbourne Hospital (where she now worked), Conyers resolved to have a standardised final exam and nursing curriculum. After her remarkable service in World War I, she maintained her interest in children and, with Matron Grace Wilson, formed the League of Former Trainees in 1921 to advocate for nurses’ education and recreational needs.
Patten was appointed director of nursing at RCH in 1982. Concerned by the increasing complexity in patient care and technologies, nursing shortages, graduate staff retention and high educational costs, Patten, with the support of the RCH committee of management, resolved to replace the undergraduate basic training school with a university-based curriculum. In 1987, after 98 years of nursing training at RCH, the last group graduated.
A paediatric graduate year was established and the existing post-basic and intensive care paediatric courses were transferred to the University of Melbourne in 1994.
Suzanne Scott
Reference: M McInness, Caring for our children: The history of nursing at the Royal Children’s Hospital, Melbourne, Melbourne: Australian Scholarly Publishing, 2006.
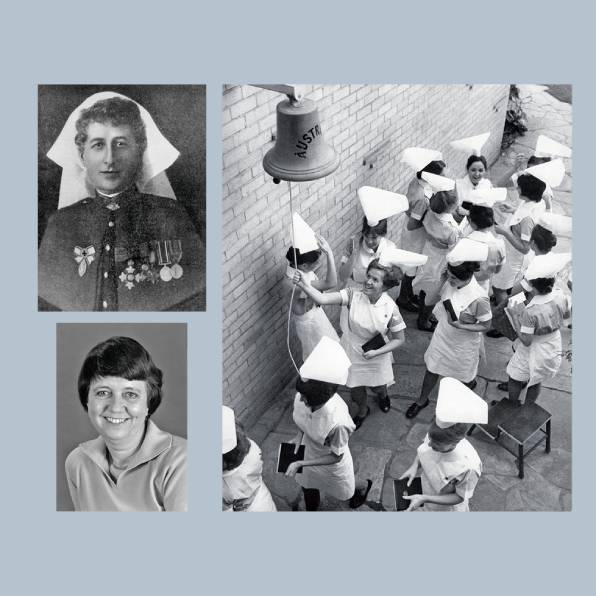
-
A pathway to paediatric physiotherapy
Physiotherapy, the Royal Children’s Hospital, and the University of Melbourne have journeyed together for more than a century. Formal education of physiotherapists in association with the University of Melbourne commenced in 1906 at the Children’s and Melbourne hospitals. The course involved medical theory and clinical practice at the university and a 12-month placement in physiotherapy practice in a recognised hospital.1
The essential contribution of physiotherapists to adult rehabilitation—through electrical modalities, exercise, massage and baths—was recognised during World War I, but the particular needs of physiotherapy for children were revealed by polio epidemics, beginning in 1908. In 1928, Dr Jean Macnamara, a medical practitioner, was appointed to oversee the Children’s Hospital’s new physiotherapy department. In 1959 she appointed Val Irwin as the first physiotherapist to head physiotherapy. Outpatients were a focus, particularly children with respiratory conditions and cerebral palsy. For the latter group, Irwin introduced innovative developmental techniques.2
The relationship between physiotherapy and the university continued to grow until the 1960s, with medical sciences taught at the university and physiotherapy subjects at Fairfield Hospital. Physiotherapy education was then transferred to Lincoln Institute of Health Sciences, but the relationship with the university continued. In 1974 Anne McCoy was appointed head of physiotherapy, which she led for three decades. McCoy was the first RCH physiotherapist to complete a Master of Science, supervised by Professors Dinah Reddihough and Terry Nolan. Her Churchill Fellowship work led to the establishment of the first paediatric gait laboratory in Australia (as discussed on pages 108–9).
The period 1976–91 saw an increase in childhood complexity and specialisation, bringing a multidisciplinary approach to child-focused care. A successful campaign followed to secure physiotherapy education at the University of Melbourne in a dedicated school of physiotherapy. For the first time, physiotherapy at RCH was funded for clinical education in line with its medical equivalent.
The strengthening of the relationship with the university has resulted in the acquisition of more postgraduate qualifications, leading to world-recognised physiotherapy research and clinical specialist roles.
Anne T McCoy AM
1 JM McMeeken, Science in our hands: Physiotherapy at the University of Melbourne 1895–2010, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, 2018.
2 P Yule, The Royal Children’s Hospital: A history of faith, service and love, Sydney: Halstead Press, 1999

-
Ninety years of social work
Isabel Hodge, having completed the inaugural Melbourne almoner (medical social work) course, started the Children’s Hospital’s Almoner Department in 1931. The hospital also trained almoner students and from 1933, when general education for social workers was established, taught students of the evolving University of Melbourne social work course.
In 1962, when Kath Dawe was appointed head of the Almoner Department, its name changed to Social Work. Dawe is remembered for her work with Dr Birrell in the 1960s, the early days of intervention in child maltreatment—until then an unrecognised phenomenon. A family bereavement service was started in 1989 by psychiatrist Julie Jones. Subsequently, bereavement programs have been provided by the Social Work Department, largely under the direction of social worker Dr Jane Sullivan, whose expertise resulted in her joining the hospital’s organ retention after autopsy team in 2020.
Between 1953 and 1982 Joyce Grant (LSE Mental Health Certificate) established psychiatric social work at RCH. In 1983 the mental health social work team was merged with the main Social Work Department, and American-trained social worker Anita Morawetz was employed as a consultant family therapist. Sarah Jones followed Morawetz and continues as a consultant in clinical supervision and culture change.
From 1990 Dr Brigid Jordan—with Dr Campbell Paul and Dr Frances Salo—was part of the internationally recognised infant mental health team, which established postgraduate infant mental health courses at the University of Melbourne. Amalgamation of the Travancore Clinic in 1992 brought a new social work team into the hospital, under the leadership of social worker and family therapist Harry Gelber. Jordan became inaugural associate professor of paediatric social work (2007–20). From 1993, during Jane Miller’s tenure as head of social work, the Aboriginal Liaison Program (see pages 144–5) underwent radical service innovation. Sarah Connolly was appointed chief social worker in 2014. She also manages the pastoral and spiritual care service and holds honorary positions in the departments of paediatrics and social work at the University of Melbourne.
Since 2016 the RCH Social Work Department has led a whole-of-hospital response to family violence and its effects on children. In 2020 COVID-19 brought increased demand as the department responded to the repercussions of the pandemic for children and families.
Dr Jane Miller AM
References: J Miller, ‘Skills, bravery, courage and foolhardiness: Seventy-five years of social work in health care in Melbourne, Australia’, Social Work in Health Care, vol. 43, nos 2/3, 2006, pp. 173–91; B Robb & J Sullivan, ‘The past and the present: Listening to parental experiences of autopsy practice’, Grief Matters, vol. 7, no. 2, 2004, pp. 39–43; C Delany et al., ‘Reflecting before, during and after the heat of the moment: A review of four approaches for supporting health staff to manage stressful events’, Journal of Bioethical Inquiry (in press).
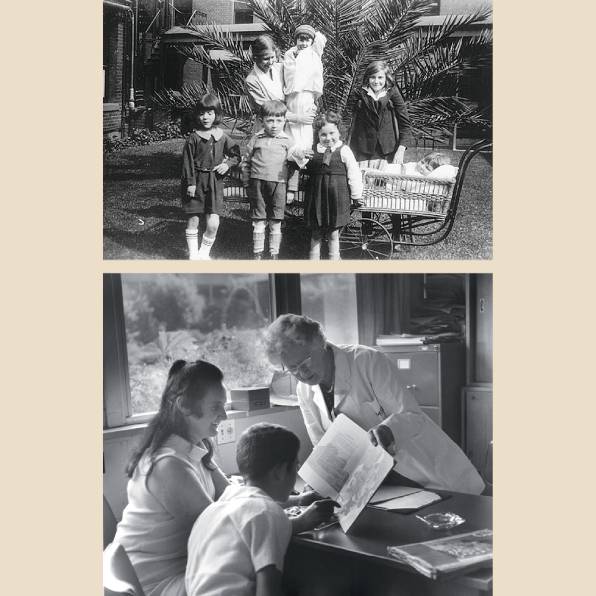
-
Speech therapy
Speech therapy at the Royal Children’s Hospital began as a service in the Department of Psychiatry in the 1930s and 1940s. During the 1950s the establishment of an outpatient plastic surgery team supported moves to independence that saw a department declared in 1984. Mirroring the tremendous growth of the profession in the 1960s and 1970s, the Speech Therapy Department contributed to international progress in the management of stuttering, articulation disorders, language difficulties, and eating problems, and in the assessment of reading and spelling.
Speech therapy as a profession in Australia changed its name to speech pathology in 1973. The introduction of four-year speech therapy degree courses in some Australian universities heralded greater capacity for dealing with a wider range of more complex paediatric conditions. Speech pathologists at the RCH worked both independently and as members of multidisciplinary teams. The department became increasingly involved in assessing and managing children with neurological conditions (congenital and acquired), craniofacial anomalies (including cleft palate and Pierre-Robin sequence), velo-pharyngeal dysfunction, swallowing disorders, and disorders of infant feeding development. The department’s work in managing neonate feeding, children before and after cardiac surgery, and children in intensive care has increased significantly. Assessment of swallowing to determine the safety and progression of oral feeding has become an important role for speech pathologists at RCH.
The RCH Speech Pathology Department was involved in the course advisory process when the University of Melbourne established its Master’s degree in speech pathology.
Technological advances have brought greater accuracy to assessment processes. Videofluoroscopic imaging has allowed speech pathologists to view the ingestion and swallowing of foods and fluids, an assessment previously possible only through clinical observation. Similarly, videofluoroscopic imaging of velo-pharyngeal function has allowed speech pathologists to provide more accurate advice on the aims and potential success of any surgical interventions. Advances in sound and imaging technology have assisted analysis and assessment of voice disorders and endoscopic assessment of the functional effects of surgery.
Bernadette O’Connor
Reference: P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999

-
Audiology
Audiology at the Children’s Hospital began, as did speech pathology, as part of the Department of Psychiatry in the 1930s and early 1940s. Miss Ruth Drake is credited with starting both services in the child guidance nursery. Drake recognised that hearing loss could contribute to behavioural disturbance or apparent developmental delay. The Audiology Department became independent of the Psychiatry Department in 1984.
The history of the Audiology Department from 1960 until 1997 is inextricably linked with Eddie Keir (pictured opposite). A trained electrical engineer and audiologist, with majors in child psychology and teaching of the deaf, Keir joined the department in 1960 and oversaw a gradual growth in staffing, being joined by a second audiologist in 1965. Keir and his colleagues recognised the need to assess a child’s capacity to hear not only isolated sounds but sounds in noise, to discriminate speech in noise, and the role of auditory processing. The department developed specialised protocols for assessing these various areas of hearing and listening. The department also pioneered techniques and processes to assess and examine children who were previously deemed untestable or too uncooperative due to behavioural or age factors. StimLab was developed in the early 1990s by the biomedical engineering team at the Royal Children’s Hospital: digital bandpass filtering of sounds familiar to children, such as the Play School theme, crying babies, barking dogs, and music, ensured accurate, frequency-specific assessments.
Developments in technology have considerably expanded the capacity to assess and give clinical advice for a much wider range of patients. For example, hearing in infants can be reliably determined via auditory brainstem response audiometry. Children undergoing oncology treatment can be monitored for the effects of any potentially ototoxic drugs used in their treatment. Middle ear function can be measured and documented via tympanometry.
The Audiology Department at RCH is a centre of excellence in paediatric assessments. Use of the best equipment, with unique features to help specialist staff identify hearing loss at a very young age, enables the department to provide a high-quality service to all children in the community.
Bernadette O’Connor
Reference: P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999.
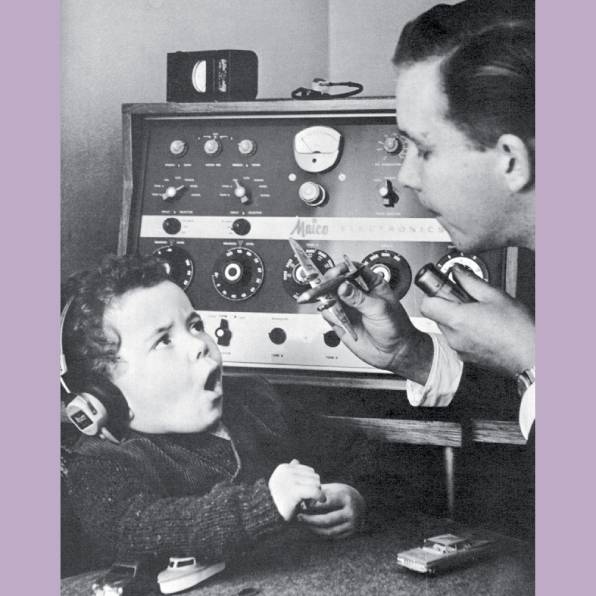
-
One hundred years of mental health care
Despite care for people’s mental health having a low community profile until recent times, when compared to that accorded to their physical health, the psychological and emotional wellbeing of children has nonetheless had a long and influential presence at RCH.1
From origins in the 1920s under Professor RJA Berry of the University of Melbourne Medical School and Dr John F Williams, the hospital’s first (and honorary) psychiatrist, along with kindergarten teacher Ruth Drake, the hospital’s care for the mental health of children has been based on a holistic framework and multidisciplinary approach. This involves understanding and treating emotionally distressed and disturbed infants, children and adolescents in the context of their families, their wider communities and their individual circumstances of health, life challenges, development, strengths and vulnerabilities.
The recognition that children often have complex and confusing inner worlds of thoughts, feelings and understanding that compromise their mental health and general development underpinned the philosophy of mental health services under the leadership of Dr Winston S Rickards. From 1955 to 1983 he further developed the team model of child psychiatry, including the allied health professions of speech pathology, audiology, psychology, child psychotherapy, social work, psychiatric nursing and teaching. Paediatricians including Professor Vernon Collins, Dr Bernard Neal and Dr Howard Williams actively supported this throughout the hospital.
Consultation liaison for hospital inpatients developed in the 1970s. Early clinics where mental health disciplines were active in medical teams included haematology and oncology, burns, and child maltreatment. In recent decades RCH has been a national leader in infant mental health, family therapy, child abuse, child trauma and community consultation. Collaborative research involving several departments and clinics reflects the hospital’s holistic and multidisciplinary approach to paediatric mental health, and has also focused on specific problems such as eating disorders and childhood anxiety.
Over the years the Royal Children’s Hospital’s mental health disciplines have provided training for child psychiatrists (the first in Australia), paediatric registrars and also, in association with the University of Melbourne and other universities, for related allied health professions.
Ruth Wraith OAM
1 L Gardiner, Royal Children’s Hospital Melbourne 1870–1970, Melbourne: Malcolm Printing, 1970, pp. 131–2; P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 557–69.
>
-
Paediatrics since 1995
The year 1995 was a turning point in the partnership between the University of Melbourne and the Royal Children’s Hospital. Until then, the Stevenson Professor and head of the Department of Paediatrics had always been on the RCH committee of management, and was a hospital administrative leader, as well as an academic leader for the RCH campus. But 1995 saw the Victorian (Kennett) government’s restructure of the Victorian hospital system in response to the recommendations of the Metropolitan Hospitals Planning Board, creating the now defunct hospital network system, which included the Women’s and Children’s Healthcare Network. Under the guidance of Professor Peter Phelan, at RCH this led to a separation of church and state: the Stevenson Professor was no longer a formal executive of the hospital. Nevertheless, leadership at RCH, including board membership of the soon to be formed Murdoch Children’s Research Institute and of the RCH Foundation, continued to be important functions for the Stevenson Chair, and remain so today.
This shift in emphasis was important for a number of reasons. Firstly, independence of academic leadership enabled strong advocacy for children first and foremost, distinct from advocacy for the campus or RCH, and simultaneously enabled the university to advocate more strongly for RCH. Secondly, academic leadership, with a push for world-class research and education on the RCH campus, would be better served. The formation of wide academic links locally, nationally and internationally, and a research vision that went beyond the walls of the hospital, assisted in achieving those goals. By 1995, the university’s Department of Paediatrics, in partnership with RCH, had embarked on an expansive program to attract professors, by offering dual hospital–university appointments, protected research time, access to students, and greater research grant opportunities, while embedding leadership in hospital departments. This transformation led to today’s strong cohort of professorial leaders on campus who strive to improve the lives of children.
Finally, the ability to provide academic and career mentorship for junior staff from medical, nursing and allied health ranks at RCH, without being in direct line management, increased the breadth and depth of support for junior staff and created many more research and educational opportunities at the hospital.
Professor Paul Monagle

-
Helping make adolescents matter
The Royal Children’s Hospital was founded to care for very young children. Yet, over the latter part of the 20th century, technological advances resulted in increasing survival of older children with complex health conditions and disabilities—including adolescents. Adolescent health had not been part of traditional paediatric training, and clinicians struggled to meet these patients’ needs.
Dr John Court (far right) was the pioneer of adolescent medicine at RCH. In the early 1980s he established a clinical program in adolescent medicine, persuaded the hospital’s committee of management to lift the upper age from 14 to 18 years, and developed an adolescent ward which recognised adolescent nursing. By the late 1980s, in response to growing community concerns about adolescent health, RCH invited up-and-coming US academic Dr Bob Blum to visit. He recommended establishing a centre for adolescent health, which would integrate research, education, clinical care and advocacy. This was achieved
in 1991 with funding from the new Victorian Health Promotion Foundation. Professor Glenn Bowes (third from right), an adult respiratory physician, was appointed inaugural director (1991–97). Based at 2 Gatehouse Street, the new Centre for Adolescent Health felt as challenging to the hospital as the age-group did for the hospital’s staff; it extended RCH clinical practices with new ways of consulting, new models of clinical care (such as peer support), and new settings for health care (for instance, clinics for homeless adolescents).
Investment in academic leadership has created many legacies: teaching in adolescent health and medicine is now mainstream for medical students and paediatric trainees; adolescent and young adult medicine is now an accredited subspecialty in Australasia; and the multidisciplinary postgraduate program in adolescent health and wellbeing at the University of Melbourne that Mary-Anne Hope, Judy Davey (fifth from left) and
Dr Michael Carr-Gregg developed still feels ahead of its time. Back in the 1990s, the young adolescent psychiatrist Dr George Patton (centre director 1998–2005) initiated a research program that quietly established the Melbourne Children’s Campus as Australia’s leading academic centre. Over the past decade these efforts have becoming globally influential, with recognition that the 2016 Lancet commission on adolescent health and wellbeing helped achieve the extraordinary framing of adolescent health in the UN’s Sustainable Development Goals.1
Professor Susan M Sawyer AM
1 Our future: A Lancet commission on adolescent health and wellbeing, Lancet, vol. 387, no. 10036, 11 June 2016.

-
Helping to build capacity in our region
From 1995 to 2011 the Royal Children’s Hospital, through RCH International, collaborated with Hanoi’s National Hospital of Pediatrics (now the Vietnam National Children’s Hospital or VNCH) in a series of training projects aimed at building capacity in administration, training and clinical skills. RCH International had earlier been commissioned by Atlantic Philanthropies to prepare a hospital services plan and functional design brief for the complete rebuilding of VNCH. Funding was provided by Atlantic Philanthropies and project management expertise by the Nossal Institute of Global Health. All levels of personnel at VNCH, from administration to project management, medical, nursing and laboratory staff, were involved in this three-year project, which was supported by the Vietnamese Ministry of Health. A significant exchange of staff between Melbourne and Hanoi took place and strong friendships developed. Among the project’s achievements were 19 directors and administration staff members gaining MBA degrees, a train-the-trainer postgraduate paediatric nursing course (continuing today), and advanced paediatric life support courses across Vietnam. Quality-assurance projects resulted in several laboratories gaining ISO accreditation. Professor Glenn Bowes, Professor Christine Kilpatrick, Mr John Stanway and dean of medicine Professor James Angus all visited Hanoi as part of the project.
Another major training project was delivered at the Cardiovascular Centre in the Hue Central Hospital. In this five-year program, 117 doctors, nurses and technical staff received training at five cardiovascular centres in Vietnam, Australia and France. Professor Dan Penny, Associate Professor Michael Cheung and Ms Mai Eames all played major roles. Professor Garry Warne AM was awarded the People’s Health Medal of the Vietnamese Ministry of Health in recognition of his role as director of these two projects.
RCH International also delivered a major three-year project to aid the recovery of a devastated regional hospital in Meulaboh, Aceh Province, Indonesia, following the 2004 Indian Ocean earthquake and tsunami. This project, funded by World Vision, was managed by the Nossal Institute of Global Health and implemented through a collaboration with the Universitas Gadja Mada in Yogyakarta. A major element was the establishment of a mental health service in Meulaboh. Professor Graeme Barnes AO initiated the collaboration and Ms Ruth Wraith OAM played a major role.
Professor Garry Warne AM
-
Occupational therapy
Occupational therapy (OT) at the Royal Children’s Hospital started in the 1930s, when the Orthopaedic Section was located at Mt Eliza (see page 117) and its patients’ average length of stay was 500 days. In OT’s early decades its main aim was to provide a ‘diversion’ for children enduring lengthy hospital stays and separation from their families. From the mid-1940s a ‘diversional therapist’ was employed at the Carlton site, but by the time of the hospital’s move to Parkville in 1963 there was a true department of five full-time therapists, who worked across many clinical areas, with burns being a specialty. During the 1960s the gradual reduction in length of inpatient stay resulted in a transition in OT services from group activities to individual treatments.
In the 1970s and 1980s OT matured as a discipline, which was reflected at RCH with the development of OT services for a broader range of children, including those recovering from surgery, cancer or head injury, or experiencing developmental disabilities or mental health problems. With an enduring goal of encouraging and developing children’s independence and mastery in their various ‘occupations’ of daily life, OT at RCH developed many areas of specialisation and expertise.
For some time, the OT department managed the hospital’s play therapy service. Now called child life therapy, this service has been a separate entity since 1982. Another major transition occurred in the late 1990s, when a dedicated research position was funded by the Parkville Auxiliary. This resulted in OTs contributing to research in areas such as neurology, developmental disability, pain, orthopaedics and plastic surgery—an involvement that continues today. Along with other allied health disciplines, OTs have developed a significant role in the assessment and diagnosis of conditions such as autism spectrum disorder, cerebral palsy and post-traumatic amnesia. The department developed the Melbourne Assessment 2, a standardised upper-limb assessment that is now sold internationally.
Occupational therapy has evolved to become an intrinsic and necessary service to RCH. Using evidence-informed practice, therapists support acute inpatients, provide expertise in specialist outpatient clinics, rehabilitation, pain management, palliative care and mental health, and through research actively contribute to the creation of new knowledge and evidence that informs paediatric practice worldwide.
Bernadette O’Connor
Reference: P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999.
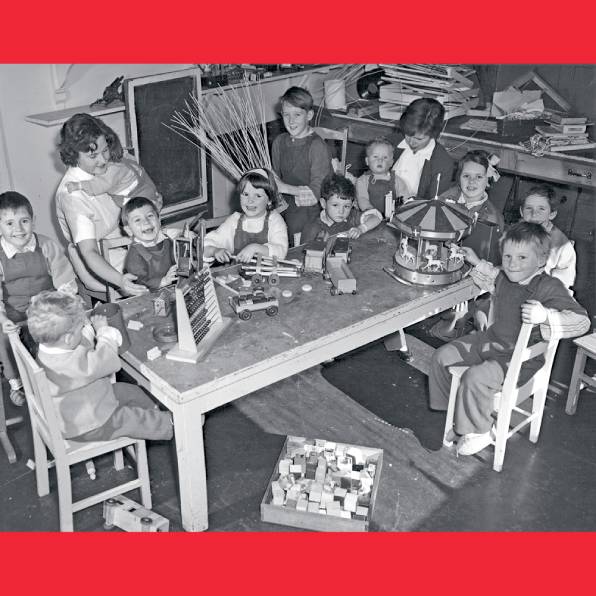
-
Prosthetics and orthotics
The origins of the Prosthetics and Orthotics Department lie in the earliest days of the Royal Children’s Hospital. Honorary surgeons arranged for splints to be manufactured
for children afflicted with tuberculosis of the bones or osteomyelitis, and in the 1920s the department was kept busy during a polio epidemic. The advent of polio vaccination and decreasing rates of tuberculosis and osteomyelitis saw the department’s workload reduce significantly in the late 1950s and early 1960s, and the making of splints was outsourced.
The department was revived in the late 1970s. The advent of plastic materials and new capacity to intervene in conditions like paraplegia and cerebral palsy led to increased staffing and new technologies. The ability to custom-mould thermoplastic orthoses for children saw the end of metal callipers, providing a more aesthetically acceptable device. In 1976 the Splint Workshop was renamed the Orthotic Department, acknowledging this wider scope and coinciding with changes in professional education, from apprenticeship to a Diploma of Health Sciences. RCH was at the forefront of these changes, running education and professional development workshops for its counterparts across Australia.
In the late 1980s, prosthetic assessment, manufacture and fitting were taken on by the department, which became the Orthotic and Prosthetic Department. It also established Australia’s first myo-electric upper-limb prosthetic program: families could procure state-of-the art ‘robotic’ hands from the department’s Limb Bank, at minimal cost.
In 2011 the department introduced 3D-imaging and CADCAM (computer-aided design and computer-aided manufacturing), purchasing a scanner and carver to shape polyurethane blocks. This was a turning point: to be able to provide advanced care for patients, superior-fitting helmets for babies with flattened heads, and safer work practices for clinicians. Scanning, CADCAM modification of scans, and 3D-carving of foam blocks have helped patients with scoliosis, allowing the creation of devices not previously possible. Technicians fabricate spinal braces using 6-kilogram foam torso models, instead of
60-kilogram plaster. These clinical and technical skills provide the digital literacy for the next step: 3D-printing, the new frontier in orthotics and prosthetics.
Bernadette O’Connor
Reference: P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999.
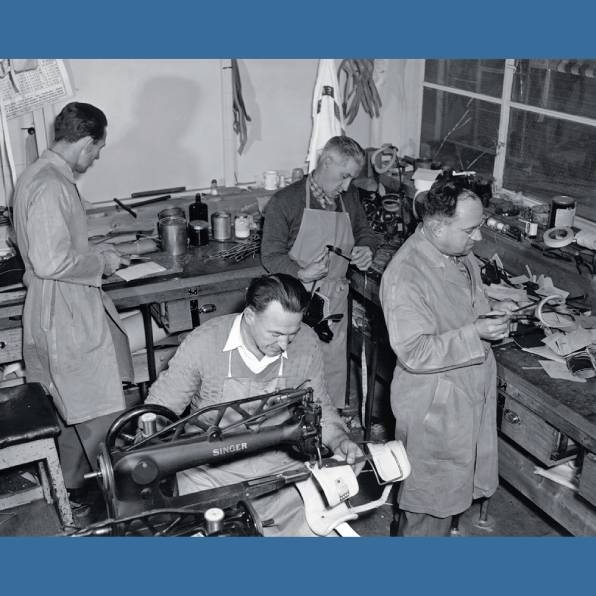
-
Clinical photography
Clinical photography began as a service at the Children’s Hospital in 1934, at both Carlton and the Orthopaedic Section at Mt Eliza. By 1938–39 all children were photographed on admission and discharge. A distinct Clinical Photography Department was established in 1948; Mr Cyril Murphy was appointed as the clinical photographer and a dedicated studio space assigned.
The service and department grew and accommodated new technologies, such as colour photography (first reported in 1942–43, but routine for decades before this). A medical artist was employed in 1967, and in 1971 the department head, Adrian Daniel, helped establish the Bachelor of Applied Science in photography at Royal Melbourne Institute of Technology.
Diversification and innovation are the hallmarks of this department. As new technologies became available, staff incorporated them to improve the clinical management of patients and support teaching and training. The latter included production of diazo slides, while the former benefited from vastly improved lighting techniques in the 1970s that enabled effective portrayal of conditions. The advent of computers revolutionised clinical photography and this evolution continues as the digitisation of numerous processes continues to change. A fully integrated digital medical information photography system was implemented in 2009.
Clinical photography has become an integral part of the multidisciplinary management of many paediatric medical conditions. With the advent of mandatory reporting of child abuse, for example, a clinical photographer remains on call to assist in collection of evidence for medical and forensic investigation. Children aged under six undergoing radiation therapy have the necessary mask prepared for them using 3D-imaging and custom manufactured by the Orthotics Department, thereby reducing trauma and avoiding the need for general anaesthesia. Surgical and non-surgical management of conditions such as craniosynostosis and pectus carinatum are not possible without this 3D-imaging service.
In research, the 3D-Imaging Centre was integral to the Australian Headshapes Examination and Analysis Database (AHEAD) project, led by RCH’s Department of Plastic and Maxillofacial Surgery, which generated a databank of 3D images of the normal craniofacial anatomy of 1,900 children.
Bernadette O’Connor
Reference: P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999.
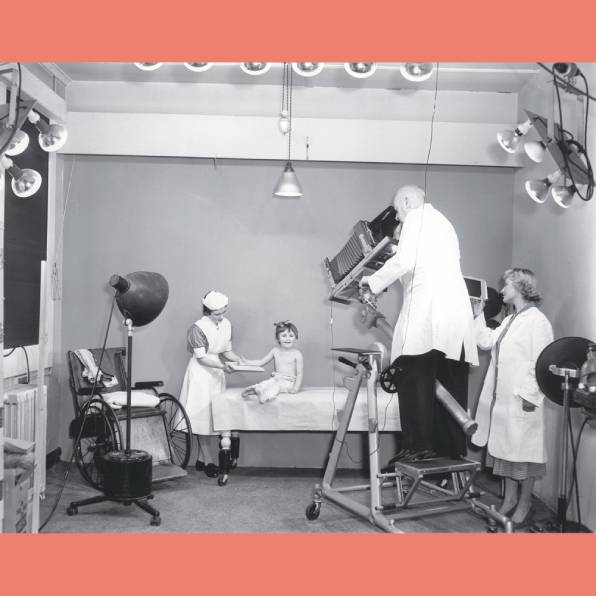
-
Turned away from care
The winter of 1881 was a very difficult and distressing time for William Barak (1824–1903), an Aboriginal leader in the Coranderrk mission near Healesville, and traditional ngurangaeta (Elder) of the Wurundjeri-willam clan. His wife, Annie, died on 8 July. His despair worsened when their only surviving son, 14-year-old David, also become gravely ill.
Barak sought the permission of the mission manager, Reverend Strickland, to take his son by coach for treatment at the Melbourne Hospital. He was granted permission and a pass. However, when they arrived at the hospital, no one was there to meet them as had been arranged. Barak carried his son to the home of Anne Fraser Bon at Kew. Mrs Bon was a long-term friend to the people at Coranderrk and later became a member of the Board for the Protection of Aborigines. She gave Barak and David a meal and took them back to the Melbourne Hospital, where at her request David was admitted. She also gave Barak a shilling for his room for the night. Barak returned to the hospital to say goodbye to David the next morning, not realising he would never see his son again, as the lad died not long afterwards.
William Barak’s experience at the Melbourne Hospital was, sadly, not unusual for Aboriginal people for more than a century. Aboriginal families visiting the nearby Children’s Hospital faced similar difficulties in obtaining care.
From the 1980s onwards, steps were taken to improve access to hospital care for Aboriginal people across Victoria. At the Royal Children’s Hospital, Rita Watkins (née Clarke) was employed as one of the first Aboriginal hospital liaison officers while I was working at the Koori Health Unit in the Victorian Health Department in 1986. She worked tirelessly for a number of years to ensure that Aboriginal families and children received better care.
Since Clarke’s time, programs such as the Wadja Aboriginal Family Place have been set up to provide welcoming and culturally safe places for Aboriginal families. The staff of programs such as this support Aboriginal and Torres Strait Islander families as they attend outpatient clinics or seek emergency care, and assist families who have a sick child in hospital. They work to ensure that Aboriginal families are supported culturally, socially and emotionally. They also advocate for Aboriginal people and promote a culturally safe hospital.
Professor Ian Anderson AO

-
Wadja Aboriginal Family Place: Equity, culture and health
The Royal Children’s Hospital’s first Aboriginal hospital liaison officer, Ruby Lako, was appointed in 1984 following the Wronski report on Aboriginal health in Victoria. Although she provided a valuable service, Lako’s role as the sole liaison officer was marginalised and could not generate the level of change that was needed.
In 1993 the establishment of a new Community Division and appointment of a new head of social work, Jane Miller, became a catalyst for change. An Aboriginal Policy Advisory Committee, the first RCH committee with Aboriginal representation, was chaired by Christine Minogue, co-director of the Community Division, and provided a forum in which senior staff and Aboriginal Elders could solve problems together. The liaison officer now had advocates at the highest level of the organisation, and in this role Robynne Nelson inaugurated the hospital’s first cross-cultural education program (1993). From 1994 Angela Clarke’s leadership developed the basis of today’s integrated, culturally safe Wadja Service. Additional philanthropic funding enabled a new way of working that recognised the need for a small cohort of Aboriginal staff and a culturally affirming stand-alone unit.1 The 1997 Bringing them home report into the Stolen Generations heralded a fundamental shift in attitudes across the hospital. The Aboriginal Family Support Unit was established in 1998, receiving several public health awards and leading change in Victorian hospitals.
In 2008 the RCH Foundation funded an improved model of care that provided case management and an Aboriginal Child Health Clinic. In 2021 Selena White, employed since 2005, has managed the team of four Aboriginal case managers. This unique service continues to evolve and lead.
Shawana Andrews and Dr Jane Miller AM
1 A Clarke, S Andrews & N Austin, Lookin’ after our own: Supporting Aboriginal families through the hospital experience, Melbourne: Aboriginal Family Support Unit, Royal Children’s Hospital, 1999; A Clarke, N Austin, S Andrews & J Miller, ‘Your way, my way: Improving access of Aboriginal children and their families to the Royal Children’s Hospital, Melbourne’, in Wendy Weeks & Marjorie Quinn (eds), Issues facing Australian families: Human services respond (3rd edn), Melbourne: Longman, 2000; A Clarke, H Goodman, N Austin, J Miller & S Andrews, ‘Promoting Koori children’s health: An affirmative approach’, Health Promotion Journal of Australia, vol. 8, no. 1, April 1998, pp. 29–33

-
The value of interpreters: Communicating with migrant communities
The Royal Children’s Hospital Interpreter and NESB Services Department offers patients and families of non-English speaking backgrounds interpreting services in more than 100 languages and dialects, to ensure that they are not disadvantaged in obtaining quality health care.
The origin of this service stems from the end of World War II: between 1945 and 1965 more than two million people emigrated to Australia.1 Hospitals and health care providers needed to adapt and evolve to serve a newly diverse and multicultural population. Until 1970, the RCH relied on multilingual volunteers, staff members and family members (including children) to communicate between NESB families and medical staff—not the ideal method for translating sensitive and complex medical information, potentially even endangering a patient’s health. Medical staff supported professionalising this service, and in 1971 hired Silvio Proy, the hospital’s first full-time interpreter. Born to Austrian and French parents, Proy came to Australia from Turkey in 1964 and was fluent in Turkish, French, Greek, Italian and Spanish. Within just a year of his appointment he had developed the interpreter service to support families on site from 9.30am to 10pm seven days a week, and via a telephone service between 10pm and 9.30am.2
For many years the department was staffed by a small team: in 1982 for instance there were just two full-time, one part-time and seven volunteer interpreters. Trained volunteers were particularly important when permanent staff went on leave. By the late 1980s Proy had helped establish the Australian Association of Hospital Interpreters, an external organisation maintaining standards and quality. He was instrumental in developing the department into what it is today, setting strict guidelines, and training and testing the interpreters to ensure ethics, cultural protocols and linguistic skills of the highest calibre. Interpreters worked closely with hospital staff, promoting the department’s services and educating colleagues on the interpreter’s role and how to communicate successfully with families from diverse cultural backgrounds.
Lucy Beattie Hughes
- National Museum of Australia, ‘Defining moments: Postwar immigration drive, 1945: Australian government announces postwar immigration drive’, nma.gov.au/defining-moments/resources/postwar-immigration-drive, updated 23 July 2021.
- LEG Sloan (medical director, RCH), All staff memo: Interpreting Service, 31 August 1972. Royal Children’s Hospital Archives and Collections Department.

-
The Gender Service
In 2003, the Royal Children’s Hospital received its first referral from a trans (transgender) young person who required medical care. In 2012, with a rise in demand for trans medicine, the service was formally established, with a multidisciplinary team led by the Department of Adolescent Medicine in collaboration with the departments of mental health, endocrinology and gynaecology. In 2015, the Victorian government provided specified funding for clinical services at the Royal Children’s Hospital Gender Service (RCHGS). In 2017, philanthropy via the RCH Foundation supported a longitudinal cohort study, known as Trans20, which formed the core of the RCHGS research program. By 2020, referral numbers had reached 473 per year and the RCHGS had established its reputation as an international leader in the field.
The RCHGS team led the creation of the inaugural Australian Standards of Care and Treatment Guidelines for Trans and Gender Diverse Children and Adolescents. First published in the Medical Journal of Australia in 2018,1 the Australian guidelines became the subject of an editorial in The Lancet endorsing its collaborative, gender-affirming approach.2
The RCHGS team also became known for its successful advocacy in improving trans rights for young people more broadly. With RCH as an independent intervenor in the case of Re Kelvin (2017), and the director of the RCHGS, Associate Professor Michelle Telfer, as the expert medical witness, the Family Court of Australia ruled to allow young people to obtain hormone treatment without the authorisation of the court in circumstances where there was no dispute. This was a landmark victory for trans rights in Australia and was included in the Federal government’s 2018 report under the United Nations Convention of the Rights of the Child.
As the RCHGS became known as an international leader in progressive, trans-friendly, child and family–focused health care, it also drew significant criticism from socially conservative individuals and organisations. This was most publicly evident through a series of more than 50 highly critical articles published in The Australian newspaper between August 2019 and mid-2021. Nevertheless, with backing from state and federal governments and the Royal Australasian College of Physicians, multidisciplinary, gender-affirming trans care continues to be offered across the country, with clinical demand continuing to grow.
Associate Professor Michelle Telfer
1 MM Telfer, K Pang, C Pace & M Tollit, ‘The creation of the Australian Standards of Care and Treatment Guidelines for Trans and Gender Diverse Children and Adolescents’, Medical Journal of Australia, vol. 209, no. 3, 18 June 2018, pp. 132–6.
2 Editorial: ‘Gender-affirming care needed for transgender children’, Lancet, vol. 391, no. 10140, 30 June 2018, p. 2576.

-
Developmental disability
The Children’s Hospital’s focus on children with disabilities dates back to the 1920s and 1930s and the establishment of the Orthopaedic Section at Mt Eliza, where young people with poliomyelitis and tuberculosis were admitted for rehabilitation.1 Between 1950 and 1967, these acquired conditions were almost eliminated, and the majority of patients had cerebral palsy, spina bifida or muscular dystrophy. When Mt Eliza closed in 1971, the Handicapped Children’s Centre was established on the Parkville campus, headed by Dr Keys Smith. The Spastic Centre begun by Dr Jean Macnamara and teacher Madge Ogilvy in the 1940s became a child assessment and treatment centre, with children attending two to four days per week. It moved from the ground floor of the hospital to a large Victorian house in North Melbourne and was renamed Uncle Bob’s Child Development Centre. In 1978 Dr John Court took over the service. He became deeply involved in the care of adolescents and, in 1986, two separate departments were formed: Court became head of adolescent medicine and Dinah Reddihough head of child development and rehabilitation.
There were urgent needs: to care for children with disabilities and their families, attract and train a workforce, raise the profile of disability on the campus, and conduct research. Most treatments were not based on evidence, and many were time and resource intensive. Over the following years research increased substantially, and the treatment of cerebral palsy in particular was revolutionised. Alternative methods of feeding, usually via gastrostomy tube, were introduced for children with aspiration and failure to thrive, Botulin toxin became a common treatment for spasticity, more invasive treatments such as intrathecal baclofen pumps and selective dorsal rhizotomy were initiated, but above all there was an increasing impetus to provide family-centred multidisciplinary care, with decisions made jointly by patient, family and providers.
In 2004, Solve@RCH was formed, a partnership between the community and the campus, resulting in the establishment of Australia’s first chair in developmental medicine, with funding from the Apex Foundation for Research into Intellectual Disability and the RCH Foundation. Subsequently a generous donation created the Lorenzo and Pamela Galli Chair in developmental medicine, further strengthening research into the causes and treatments of developmental disability.
Professor Dinah Reddihough AO
1 P Yule, The Royal Children’s Hospital: A history of faith, science and love, Sydney: Halstead Press, 1999, pp. 196–7.

-
Responding to abused children and sexual assault
The Royal Children’s Hospital Child Protection Unit, staffed with one doctor, three social workers, a nurse, and part-time psychologist and psychotherapist, was established in 1986. Later becoming the Gatehouse Centre, the focus was on care for children in the context of their family. Numerous legislative, systemic and funding changes over the years have seen the Gatehouse staff grow to more than 30, including art therapists, nurses, psychologists and social workers, plus a part-time neuropsychologist, occupational therapist and psychiatrist to respond to the ever more complex needs of the children who attend.
It was, however, a 4 Corners and The Age series, ‘Our children, our shame’,1 and the Fogarty Report,2 that brought the existence of child sexual abuse boldly to the public’s attention. Mandatory reporting of child abuse was first legislated in the Children and Young Persons’ Act 1989, sparking an increase in children identified as needing a therapeutic response, not just a child welfare or justice response. The Victorian Law Reform Commission continued developing responses to child sexual abuse, recommending, in 2004, 302 improvements to legal responses to child sexual abuse and creating the Child Witness Service.
Our therapeutic work with children and young people has developed significantly. Better recognition of the effects of trauma on children saw the emergence of new, trauma-focused therapies, while the Children, Youth and Families Act 2005 introduced therapeutic treatment orders for young people with problem sexual behaviour. Service provision has diversified: in addition to assessment, treatment, advocacy and outreach, the Gatehouse provides education and training and undertakes research. Since the 2013 Royal Commission into Institutional Responses to Child Sexual Abuse,3 demand for services has continued to grow, and an understanding of the importance of collaborative, trauma-informed services that meet our clients where they are, has become central to all that the Gatehouse Centre provides.
Karen Hogan and Dr Helen Kambouridis
1 ‘Our children, our shame’, The Age, May 1988.
2 JF Fogarty, Protective services for children in Victoria: A report, Melbourne: Child Protection Services Branch, Community Services Victoria, 1993.
3 Royal commission into institutional responses to child sexual abuse, Commonwealth of Australia,

-
Joey’s book
A Royal Children’s Hospital prescription booklet dating back to the 1960s remains a prompt for memories, while also speaking profoundly about another time.
Melbourne is threaded together by stories of immigration: people who have arrived here by choice or by chance. The story of the De Feudis family reflects both choice and chance. Woven into that narrative is the path to the RCH and the legacy of a child born seriously unwell.
Arriving in this world on 10 September 1954, on what should have been a joyous occasion, Joseph Bernard (Joey) De Feudis was born with cardiac and structural anomalies, and it was predicted that he would not reach adolescence. For mother Josephine, the language barrier was impenetrable, so power and language remained in the hands of the father, Michael. As an Italian farming soldier captured overseas during World War II and brought to work on a farm in South Gippsland, he had been taught to read, write and speak English. But even with his language skills, he too became frightened and hoped that Joey’s illness would just disappear. It was never spoken of, its consequences unknown, and, as Joseph grew up with two younger siblings, the need to confront the ‘illness’ was too overwhelming for the parents.
Sadly, Joey was not to know about his condition until, as a young man embarking on his first job in a bank, he underwent a medical examination. The stunned doctor announced to Joseph that his heart was on the wrong side. This shocking revelation changed him. Suddenly, he understood the past: the trips to the RCH, the scars where catheters had penetrated, his exclusion from sports, and why, when he was puffed out, his lips would turn blue.
The silence imposed upon Joseph about his condition was meant to protect him. But, when he was 24, a dentist’s appointment resulted in a fatal combination: dentistry, cardiac problems and severe infection. This connection was not well understood in 1978 and, in November of that year, Joseph died suddenly while a patient at the Alfred Hospital.
Joey’s was a life cut short, but it was also a life prolonged by many trips along the road from South Gippsland to the Royal Children’s Hospital in Parkville.
Anne Rahilly

-
The Teddy Bear Hospital
The Teddy Bear Hospital (TBH) is a volunteer student initiative established in 2009. This collaboration between the Royal Children’s Hospital and the University of Melbourne is a unique educational program that benefits both children and health care students. It is coordinated by a 60-member committee of students from across the Faculty of Medicine, Dentistry and Health Sciences, and is overseen by Professor Paul Monagle of the Department of Paediatrics.
The TBH has two main aims: firstly, to demystify health care for children through positive imaginative play with their bears, and secondly, to provide opportunities for students to develop their paediatric communication skills. It is a delight to see kids with their bears, interacting with health professionals, and returning year after year. We consistently observe that after even one event, students’ confidence in interacting with kids grows significantly, and we receive feedback to this effect from the students themselves.
We create an entire hospital experience, with services ranging from radiology, pathology and nursing to dentistry and physiotherapy—and more. The children take their bears through these services, guided by students. All our equipment has been handcrafted by our student committee over the years. Our two major annual events are the Good Friday Appeal and the Chadstone Winter Check-up. Typically we will welcome some 2,000–3,500 kids, and involve up to 1,200 students. We proudly contribute all the funds raised from our ticket and bear sales towards supporting the excellent work of the RCH. We also conduct events at metropolitan and rural kindergartens and primary schools, community centres and the Victorian Aboriginal Health Service.
The RCH is the team’s base for meetings, volunteer training and equipment storage. The RCH is also one of Melbourne Medical School’s sites for paediatric placement, and the TBH has become a regular part of the placement experience—a powerful recognition of its value.
The TBH program is a mammoth effort by the student cohort, but we could not do it all on our own. We receive support from many organisations, including VISY, Emergency Services, our venues—the Melbourne Convention and Exhibition Centre and Chadstone shopping centre—the University of Melbourne and RCH. We are deeply grateful to them all.
Chelsea Xu and Kate Wishart
-
Philanthropic leadership: The Royal Children’s Hospital Foundation
Philanthropy has been a part of the Royal Children’s Hospital since the very beginning. Founding doctors William Smith and John Singleton had a vision in 1870 ‘to help sick and injured children free of charge’.
In 1989 this philanthropic spirit was formalised when the hospital’s committee of management established the Royal Children’s Hospital Foundation. Initially set up as a trust to secure donated funds and show donors the benefits of their support, it soon developed into a nationally renowned fundraising organisation. The Royal Children’s Hospital Foundation brings together supporters from across Australia, including community fundraisers, corporations, bequests, trusts and foundations, as well as our dedicated Auxiliaries and the Good Friday Appeal.
From relatively modest beginnings (raising some $2 million in 1989), the Royal Children’s Hospital Foundation has grown significantly, thanks to this dedicated community that rallies together to support world-leading care for patients at the hospital. In 2019 alone, the foundation raised a remarkable $62.3 million. This immense generosity has helped make the Royal Children’s Hospital a pre-eminent institution. While the Victorian government funds the hospital’s operating costs, donations enable medical excellence that otherwise would not be possible. The programs and initiatives funded by donated money go above and beyond the hospital’s day-to-day activities. They take the Royal Children’s Hospital from being a good hospital to a great one.
For 32 years, the Royal Children’s Hospital Foundation has supported thousands of initiatives, based on four pillars: leadership, education and training; patient and family–centred care; equipment and technology; and ground-breaking research. Thanks to this community support, innovation has been made possible on campus through such pioneering projects as the establishment of the Victor and Loti Smorgon Chair in paediatrics, the Gender Service, Wadja Aboriginal Family Place, the electronic medical record system, and the purchase of the intraoperative magnetic resonance imaging system.
The Royal Children’s Hospital Foundation continues to inspire the community to invest in the hospital and its campus partners, to transform children’s health today and into the next 150 years.
Sue Hunt

-
The joys of paediatrics
Since 1879, the Royal Children’s Hospital has played host to thousands of medical students taking their first dip into the world of paediatric medicine. Trepidation quickly gives way to a sense of excitement and privilege, as students are guided through the unique aspects of caring for children, learning that they are anything but ‘little adults’, and what to do when eventually faced with a crying patient. During their first week, students are given a crash course in developmental milestones, the 4-2-1 rule of maintenance fluid, and all the paediatric-specific conditions that they will be quizzed on during morning rounds.
Although many of the students who train at the Royal Children’s Hospital ultimately will not become paediatricians, their time spent learning paediatric medicine is anything but wasted. A large proportion will continue to work with children in their chosen field, such as general practice or emergency medicine, but, more importantly, we hope they will take on the characteristics that paediatricians embody in their daily practice. Holistic, patient-centred care that considers both the individual and their family is a fundamental tenet that students are taught during their placement at the Royal Children’s Hospital, and can be applied to any medical specialty.
Personally, I have countless fond memories of my time at the Royal Children’s Hospital. From looking after twin boys sick with bronchiolitis so that their mother could get some sleep, to being taught the fastest way to complete a Legend of Zelda video game by one of the patients on the adolescent ward, no day was ever the same. The paediatricians, nursing staff and allied health team were patient and encouraging in the education of every medical student, ensuring that we all built up confidence in caring for children.
The joys of studying paediatric medicine lie not only in being given the privilege of caring for the most special and delightful group of patients that medicine has to offer, but also in the tireless and unwavering support provided by staff, every day.
Dr Kieren Fahey

-
The power of partnerships: The future of community child health
Sometimes, to look forward, it is important to look back. The Royal Children’s Hospital’s vision of ‘Great Care, Everywhere’ has its origins in a department established more than 25 years ago, which focused on meeting the needs of children in the context of their family and community. The Centre for Community Child Health, driven by the partnership of founding director Professor Frank Oberklaid and deputy director Associate Professor Jill Sewell, led the way in treating what were then the ‘new morbidities’ of developmental and behavioural paediatrics. Their patients were children who required not hospital beds, but well-trained paediatricians who understood the community context. Perhaps even more radical at the time was the emphasis on equity, prevention, early intervention and the application of evidence to policy, practice and parenting.
Well ahead of its time, the Centre has led many influential statewide and national initiatives, including the Australian Early Development Census, the Victorian Infant Hearing Screening Program, right@home, and the Raising Children Network. This is knowledge translation in action.
The Centre’s purpose is that every child thrives. To achieve this, its unique structure supports innovative research, provides specialist developmental and behavioural clinics and paediatric training, delivers infant hearing screening for all Victorian babies, and is at the vanguard of translating evidence into action. Fundamental to its success is collaboration. By working with children, families, practitioners, communities and government, the Centre can better ensure that decisions are based on evidence, and can reform systems and services to provide better experiences and environments for children.
As RCH commemorates its 150th anniversary, we are in a time of unprecedented turmoil—one that magnifies the disparities in our community. Now more than ever, the Centre is pursuing equitable health, development and wellbeing for all Australian children, and will continue to play a unique and integral role at RCH. We aim to provide and inspire the best care, everywhere, now and into the future.
Professor Sharon Goldfeld

-
Telehealth for children
The COVID-19 pandemic has delivered a transformative shock to health care systems, bringing many changes to the ways in which clinicians deliver care, and to consumers’ preferences. As part of this transformation, the Australian government’s public health insurance scheme (Medicare) relaxed geographical constraints on patients’ entitlement to reimbursement for video consultations, and for the first time introduced Medicare payment for telephone consultations for all patients, not just those living in rural and regional areas.
While telehealth may be preferable for some consumers, it may not be preferred by all of them, all of the time. Reasons why some people prefer telehealth and others do not are unclear. So we surveyed 2,436 caregivers of children attending the Royal Children’s Hospital outpatient clinics, asking for their views on telehealth consultations for their child, preference over in-person consultations, and potential cost savings, categorised by the child’s condition and their family’s socio-economic status and location.
We surveyed caregivers between 3 June and 25 August 2020. Most found telehealth consultations convenient, acceptable, safe and private, and capable of answering their questions and concerns. However, caregivers who spoke a language other than English, and those of patients attending for behavioural, mental health, developmental or other concerns (such as allied health), were more likely to prefer in-person consultations over telehealth. Reported cost savings on caregiver time averaged $144.98 per family per consultation, while cost savings on transport averaged $84.90 per family per consultation. Cost savings were greatest for families living in low and middle socio-economic areas and regional or rural areas, highlighting the potential role of telehealth in reducing inequity by improving access to care for poorer or regional families.
Thus, while paediatric telehealth video consultations are largely viewed favourably by caregivers, they may not be the best way to offer care for children with behavioural, mental health or developmental difficulties. Our findings can help inform the design of health policy on availability of telehealth consultations as part of the mix of services provided by the Australian health system.
Professor Harriet Hiscock
Reference: H Hiscock, R Pelly, X Hua, S West, D Tucker, C-M Raymondo & K Dalziel, ‘A survey of paediatric telehealth benefits from the caregiver perspective’, Australian Health Review, 2021

-
Looking forward, looking back
For 150 years, the Royal Children’s Hospital has provided excellent health care to children and young people in Melbourne and Victoria, and even across Australia. Upon reaching this milestone we can reflect on the achievements, innovations and challenges of the past 150 years, and chart a roadmap for the future that will increase our capacity to improve paediatric health care at the RCH and beyond.
We have already made excellent progress in transforming the RCH into a digital hospital—responding to a need that has been exacerbated by the COVID-19 pandemic and the disruption it has caused to our services. It is in part through this disruption that we have recognised the need to take greater strides towards adopting virtual methods of health care.
Over the next five years, the RCH will implement a virtual care strategy to help us achieve our aim of delivering ‘Great Care, Everywhere’. This will use digital and telecommunications technology as we provide continuous, connected and coordinated care for our patients and their families. These new models of care will take the form of telehealth, digital care coordination and remote monitoring, linking together patients, clinicians and the wider community, to allow patient care to be accessible from home and in the community, as well as in hospital. The future of health care lies in providing services outside the walls of the hospital, with an inspired workforce, community, patients and families working together under our virtual care philosophy, applying innovative models of care and technology to achieve better results for patients. Ultimately, our vision is to use virtual care technology to offer the best care, in the best place, at the right time.
Importantly, the opportunities we have before us are immense—not only in the adoption of digital technologies to deliver care, but also in where this great institution could lead paediatric health care in the future. Let us build on our rich history and the foundations we have laid over the past 150 years to continue our work in being a great children’s hospital, leading the way for the benefit of generations to come.
The Hon. Rob Knowles AO
-
Richard I Woodman England (1784–1859)
Richard I Woodman England (1784–1859) The idle and luxuriant student attended at his apartment in the college by his sempstress. From The Idler 1798 stipple engraving on paper Baillieu Library Print Collection, The University of Melbourne Gift of Dr J Orde Poynton 1959 1959.5536.000.000